

Benign acute children myositis: 5 years experience in a tertiary care pediatric hospital
- PMID: 37462800
- PMCID: PMC10587191
- DOI: 10.1007/s00431-023-05115-9
Benign acute children myositis: 5 years experience in a tertiary care pediatric hospital
Abstract
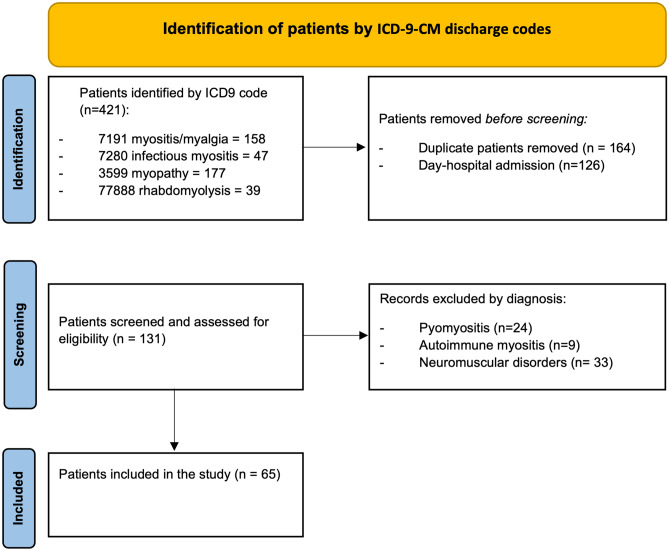
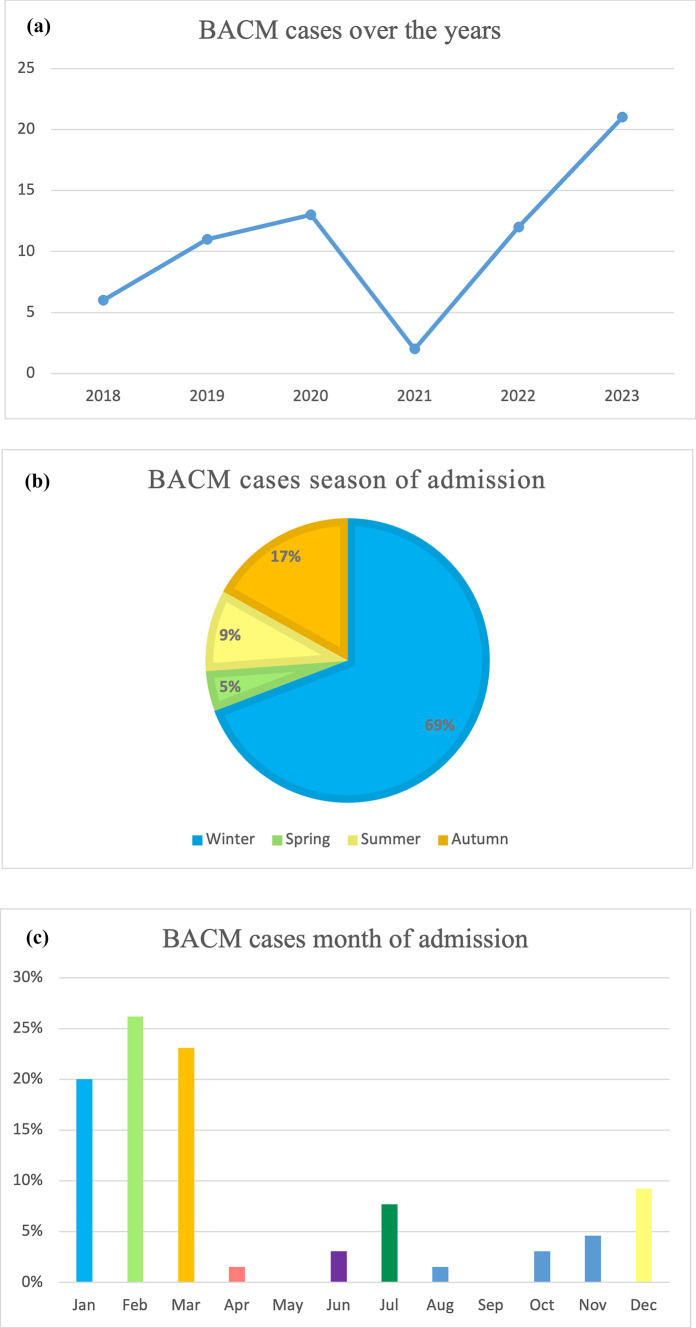
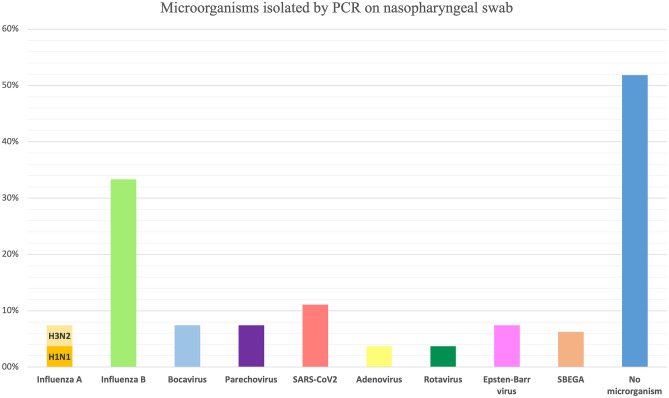
Benign acute childhood myositis (BACM) is a self-limited childhood illness, and viral infections mainly cause it. Clinical and laboratory alterations usually normalize rapidly; generally, the only medical intervention required is supportive (hydration and analgesic medication). The low awareness about BACM often led to delayed diagnosis and unneeded ancillary investigations. This study aims to better characterize the clinical and laboratory features of BACM to improve the diagnostic process and inpatient and outpatient management. We conducted a retrospective study selecting all children admitted to Meyer's Children's Hospital-IRCCS (Florence, Italy) with a diagnosis of BACM over the last 5 years, both those visited at Emergency Department (ED) and those admitted to the Pediatric Unit. Clinical, laboratory, and instrumental data were collected from electronic clinical records and analyzed. Overall, sixty-five patients were enrolled; 49 children were visited and discharged directly from ED, whereas 16 were admitted in the Pediatric or Neurologic Wards. The median age was 6.56 years (IQR 4.9-9.1). Male gender (66.1%) and Caucasian ethnicity (70%) were prevalent. Most patients were admitted during winter, and a second peak was found in autumn. All patients had bilateral calf pain, most of them (87.7%) associated with asthenia and refuse to walk (93.8%). Prodromal symptoms were fever (75.3%), cough (32.3%), coryza (26.1%), sore throat (26.1%), and vomiting (15.3%). The median value of CPK was 1827 U/L (IQR 915.5-2462) at peak. CPK median time to normalization was 7 days (IQR 7-8.5) from the nadir. Influenza B was the virus most frequently BACM associated, followed by Influenza A; a novel association with Sars-CoV-2 has been detected. Two patients had pathogenic variants at the Next Generation Sequencing myopathies panel. Conclusion: School-aged children admitted to the hospital with walking difficulty and myalgia, generally after an upper respiratory tract infection with a moderate CPK elevation, should remind at first of BACM. Rapid complaint resolution and biochemical markers normalization will prevent unnecessary tests and inappropriate therapies. What is Known: • BACM is a self-limited syndrome associated with acute infections. Influenza A and B viruses are the main etiological agents, but BACM may be related to many other microorganisms like Parainfluenza virus, Epstein-Barr virus, Cytomegalovirus, Human herpesvirus 6, Respiratory syncytial virus, Coxsackieviruses, Mycoplasma pneumoniae, Streptococcus pyogenes, Legionella, and Salmonella spp. • Clinical and laboratory alterations usually normalize rapidly; generally, the only medical intervention required is supportive (hydration, analgesic medication). Evolution in rhabdomyolysis and kidney damage is possible but rarely reported. What is New: • Sars-CoV-2 could be an emerging possible cause of BACM. During and after the Sars-CoV-2 outbreak, virus infection seasonality has changed, and so has BACM seasonality. • Screening tests for muscular and metabolic disorders are recommended in recurrent myositis and/or cases with marked CPK elevation (≥ 5000 U/L).
Keywords: Benign myositis; Children; Gait complaint; Influenza; Myalgia; Pediatrics.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Öztürk B, Göktuğ A, Bodur İ, Yaradılmış RM, Güneylioğlu MM, Güngör A, Tekeli A, Akca Çağlar A, Karacan CD, Tuygun N (2022) Benign acute childhood myositis: factors associated with muscle symptoms and resolution. Pediatr Int 64(1):e15273. 10.1111/ped.15273. PMID: 36321340 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
