

Rationale and evidence for the use of new beta-lactam/beta-lactamase inhibitor combinations and cefiderocol in critically ill patients
- PMID: 37462830
- PMCID: PMC10354316
- DOI: 10.1186/s13613-023-01153-6
Rationale and evidence for the use of new beta-lactam/beta-lactamase inhibitor combinations and cefiderocol in critically ill patients
Abstract
Background: Healthcare-associated infections involving Gram-negative bacteria (GNB) with difficult-to-treat resistance (DTR) phenotype are associated with impaired patient-centered outcomes and poses daily therapeutic challenges in most of intensive care units worldwide. Over the recent years, four innovative β-lactam/β-lactamase inhibitor (BL/BLI) combinations (ceftolozane-tazobactam, ceftazidime-avibactam, imipenem-relebactam and meropenem-vaborbactam) and a new siderophore cephalosporin (cefiderocol) have been approved for the treatment of certain DTR-GNB infections. The literature addressing their microbiological spectrum, pharmacokinetics, clinical efficacy and safety was exhaustively audited by our group to support the recent guidelines of the French Intensive Care Society on their utilization in critically ill patients. This narrative review summarizes the available evidence and unanswered questions on these issues.
Methods: A systematic search for English-language publications in PUBMED and the Cochrane Library database from inception to November 15, 2022.
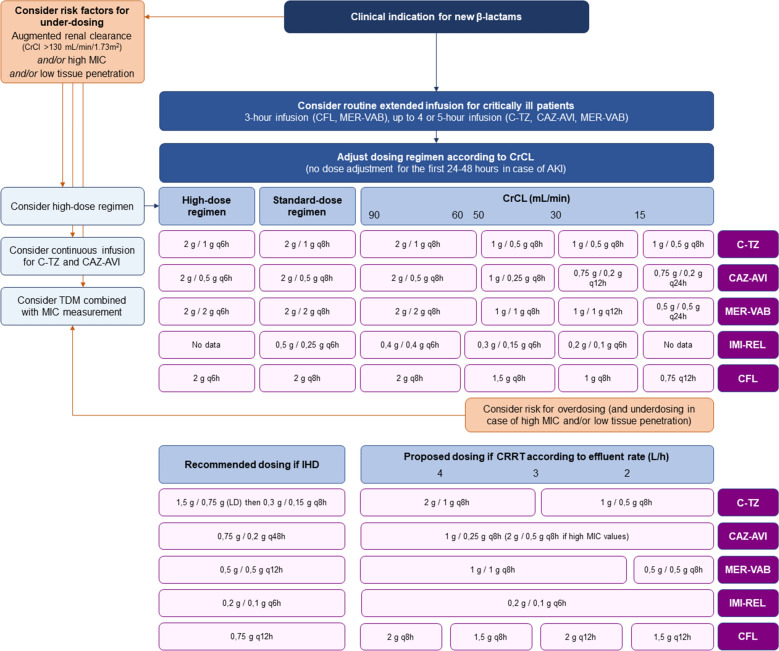
Results: These drugs have demonstrated relevant clinical success rates and a reduced renal risk in most of severe infections for whom polymyxin- and/or aminoglycoside-based regimen were historically used as last-resort strategies-namely, ceftazidime-avibactam for infections due to Klebsiella pneumoniae carbapenemase (KPC)- or OXA-48-like-producing Enterobacterales, meropenem-vaborbactam for KPC-producing Enterobacterales, ceftazidime-avibactam/aztreonam combination or cefiderocol for metallo-β-lactamase (MBL)-producing Enterobacterales, and ceftolozane-tazobactam, ceftazidime-avibactam and imipenem-relebactam for non-MBL-producing DTR Pseudomonas aeruginosa. However, limited clinical evidence exists in critically ill patients. Extended-infusion scheme (except for imipenem-relebactam) may be indicated for DTR-GNB with high minimal inhibitory concentrations and/or in case of augmented renal clearance. The potential benefit of combining these agents with other antimicrobials remains under-investigated, notably for the most severe presentations. Other important knowledge gaps include pharmacokinetic information in particular situations (e.g., pneumonia, other deep-seated infections, and renal replacement therapy), the hazard of treatment-emergent resistance and possible preventive measures, the safety of high-dose regimen, the potential usefulness of rapid molecular diagnostic tools to rationalize their empirical utilization, and optimal treatment durations. Comparative clinical, ecological, and medico-economic data are needed for infections in whom two or more of these agents exhibit in vitro activity against the causative pathogen.
Conclusions: New BL/BLI combinations and cefiderocol represent long-awaited options for improving the management of DTR-GNB infections. Several research axes must be explored to better define the positioning and appropriate administration scheme of these drugs in critically ill patients.
Keywords: Aztreonam; Carbapenem resistance; Cefiderocol; Ceftazidime–avibactam; Ceftolozane–tazobactam; Enterobacterales; Imipenem–relebactam; Intensive care unit; Meropenem–vaborbactam; Pseudomonas aeruginosa.
© 2023. The Author(s).
Conflict of interest statement
FB declares having received lecture and consulting fees from MSD, lecture fees for BioMérieux and conference invitation from Pfizer. SH declares having received a conference invitation from Shionogi and lecture fees from Pfizer. OP declares having received consulting fees and conference invitation from MSD, and conference invitation from Correvio. JP declares having received lecture fees from Gilead. JRZ declares having received lecture fees from MSD, Pfizer, Shinogi and BioMérieux, and conference invitations from MSD and Pfizer. All other authors declare having no potential conflict of interest related to this article.
Figures
References
-
- Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America guidance on the treatment of extended-spectrum β-lactamase-producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa) Clin Infect Dis. 2021;72(7):e169–e183. doi: 10.1093/cid/ciaa1478. - DOI - PubMed
-
- Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America guidance on the treatment of AmpC β-lactamase-producing Enterobacterales, carbapenem-resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia infections. Clin Infect Dis. 2022;74(12):2089–2114. doi: 10.1093/cid/ciab1013. - DOI - PubMed
-
- Paul M, Carrara E, Retamar P, Tängdén T, Bitterman R, Bonomo RA, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine) Clin Microbiol Infect. 2022;28(4):521–547. doi: 10.1016/j.cmi.2021.11.025. - DOI - PubMed
-
- Rosenthal VD, Bat-Erdene I, Gupta D, Belkebir S, Rajhans P, Zand F, et al. International Nosocomial Infection Control Consortium (INICC) report, data summary of 45 countries for 2012–2017: Device-associated module. Am J Infect Control. 2020;48(4):423–432. doi: 10.1016/j.ajic.2019.08.023. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
