

Effect of belimumab on kidney-related outcomes in patients with lupus nephritis: post hoc subgroup analyses of the phase 3 BLISS-LN trial
- PMID: 37463054
- PMCID: PMC10689192
- DOI: 10.1093/ndt/gfad167
Effect of belimumab on kidney-related outcomes in patients with lupus nephritis: post hoc subgroup analyses of the phase 3 BLISS-LN trial
Abstract
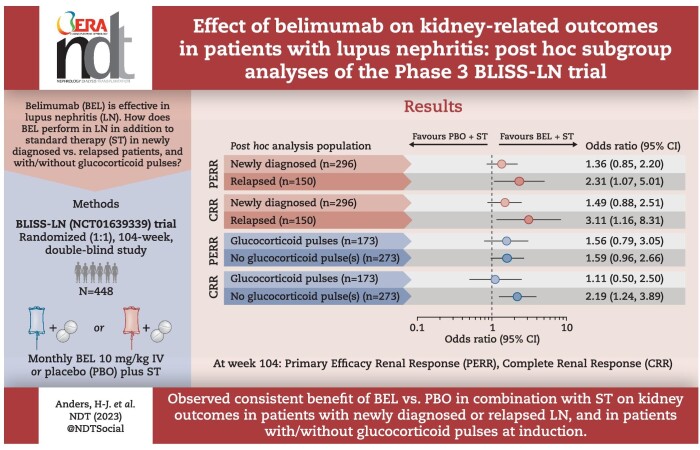
Background: Data on belimumab efficacy in patients with lupus nephritis (LN) according to diagnosis duration or induction therapy are limited. Post hoc analyses of the phase 3, randomized, double-blind BLISS-LN study (GSK BEL114054; NCT01639339) were performed to assess belimumab efficacy on kidney-related outcomes in newly diagnosed and relapsed LN subgroups and according to the use of glucocorticoid (GC) pulses at induction.
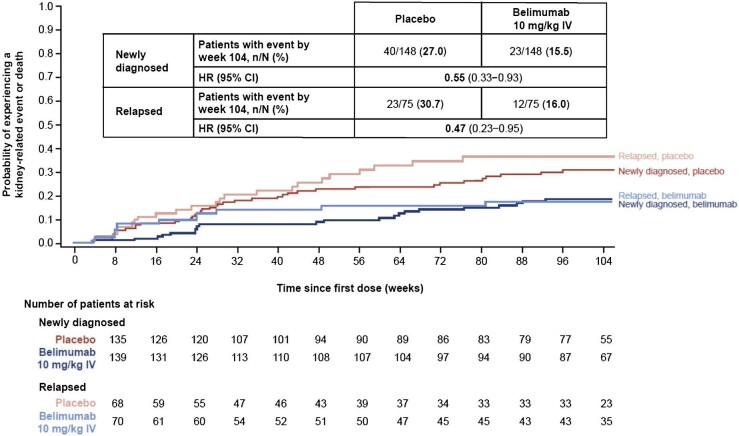
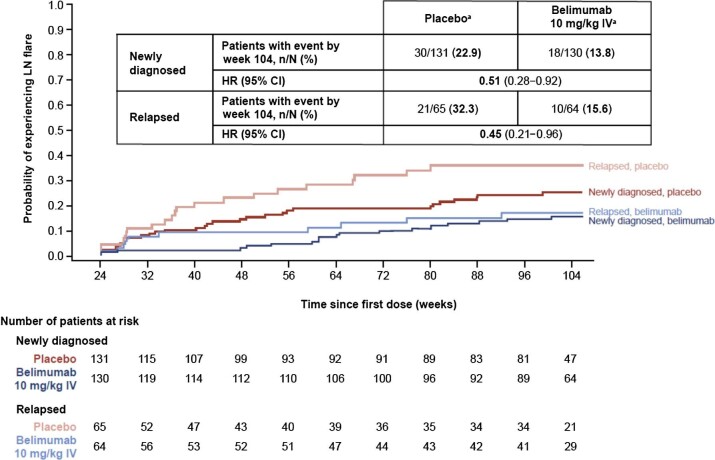
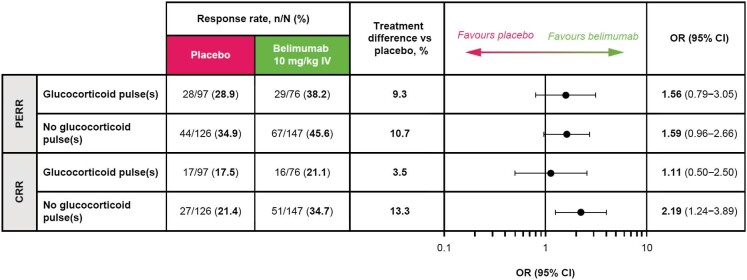
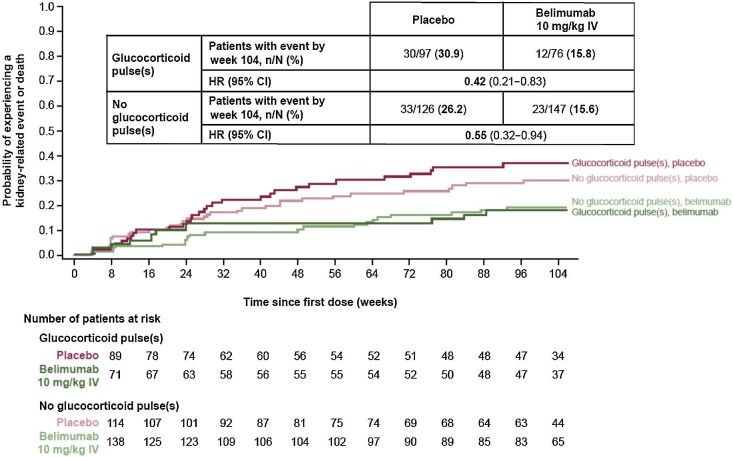
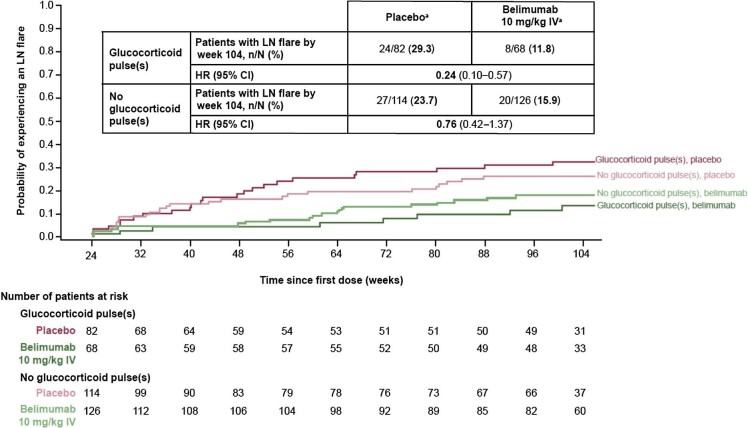
Methods: BLISS-LN randomized 448 patients with active LN to monthly intravenous belimumab 10 mg/kg or placebo plus standard therapy. Post hoc analyses assessed primary efficacy renal response (PERR) and complete renal response (CRR) at week 104, time to kidney-related event or death and time to first LN flare from week 24 in newly diagnosed and relapsed patients and patients with/without GC pulses at induction.
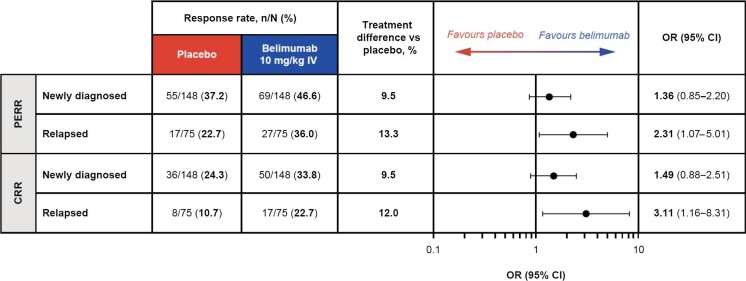
Results: A greater proportion of patients achieved a PERR with belimumab versus placebo in the newly diagnosed {69/148 [46.6%] versus 55/148 [37.2%]; odds ratio [OR] 1.36 [95% confidence interval (CI) 0.85-2.20]} and relapsed [27/75 (36.0%) versus 17/75 (22.7%); OR 2.31 (95% CI 1.07-5.01)] subgroups. Similarly for CRR [newly diagnosed: 50/148 (33.8%) versus 36/148 (24.3%); OR 1.49 (95% CI 0.88-2.51) and relapsed: 17/75 (22.7%) versus 8/75 (10.7%); OR 3.11 (95% CI 1.16-8.31)]. The probability of kidney-related event or death, or LN flare was lower with belimumab versus placebo in both subgroups. Belimumab was associated with improved kidney outcomes versus placebo with or without GC pulses at induction.
Conclusion: Data suggest consistent benefits of belimumab on kidney outcomes for newly diagnosed and relapsed patients, and irrespective of GC pulses at induction.
Keywords: B cells; belimumab; glucocorticoids; lupus nephritis; proteinuria.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
H.-J.A. has received consultancy fees or honoraria from AstraZeneca, Bayer, Boehringer, GSK, Idorsia, Janssen, Kezar, Sanofi, Otsuka, Novartis and PreviPharma; is a member of the Scientific Advisory Board of the European Renal Association and an associate editor at
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
