

Clinical impact of OCT-derived suboptimal stent implantation parameters and definitions
- PMID: 37463223
- PMCID: PMC10735315
- DOI: 10.1093/ehjci/jead172
Clinical impact of OCT-derived suboptimal stent implantation parameters and definitions
Abstract
Aims: Despite growing evidence supporting the clinical utility of optical coherence tomography (OCT) guidance during percutaneous coronary interventions (PCIs), there is no common agreement as to the optimal stent implantation parameters that enhance clinical outcome.
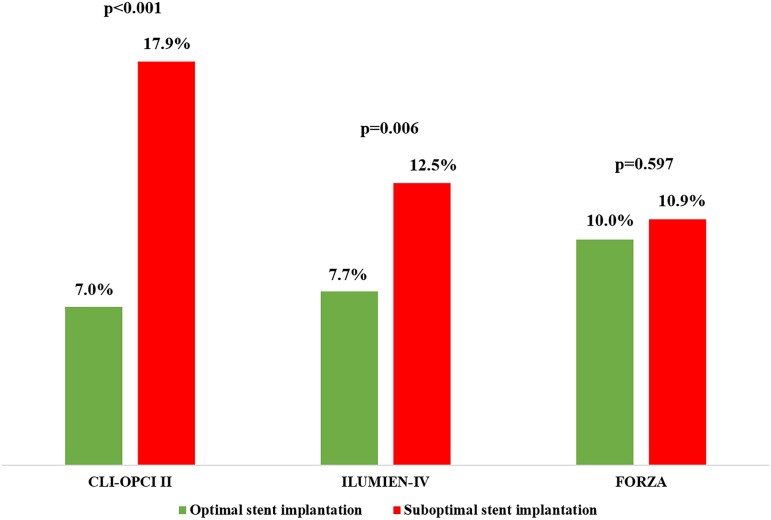
Methods and results: We retrospectively examined the predictive accuracy of suboptimal stent implantation definitions proposed from the CLI-OPCI II, ILUMIEN-IV OPTIMAL PCI, and FORZA studies for the long-term risk of device-oriented cardiovascular events (DoCE) in the population of large all-comers CLI-OPCI project. A total of 1020 patients undergoing OCT-guided drug-eluting stent implantation in the CLI-OPCI registry with a median follow-up of 809 (quartiles 414-1376) days constituted the study population. According to CLI-OPCI II, ILUMIEN-IV OPTIMAL PCI, and FORZA criteria, the incidence of suboptimal stent implantation was 31.8%, 58.1%, and 57.8%, respectively. By multivariable Cox analysis, suboptimal stent implantation criteria from the CLI-OPCI II [hazard ratio 2.75 (95% confidence interval 1.88-4.02), P < 0.001] and ILUMIEN-IV OPTIMAL PCI [1.79 (1.18-2.71), P = 0.006] studies, but not FORZA trial [1.11 (0.75-1.63), P = 0.597], were predictive of DoCE. At long-term follow-up, stent edge disease with minimum lumen area <4.5 mm2 [8.17 (5.32-12.53), P < 0.001], stent edge dissection [2.38 (1.33-4.27), P = 0.004], and minimum stent area <4.5 mm2 [1.68 (1.13-2.51), P = 0.011] were the main OCT predictors of DoCE.
Conclusion: The clinical utility of OCT-guided PCI might depend on the metrics adopted to define suboptimal stent implantation. Uncovered disease at the stent border, stent edge dissection, and minimum stent area <4.5 mm2 were the strongest OCT associates of stent failure.
Keywords: clinical research; drug-eluting stent; optical coherence tomography; risk stratification.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: G.B.-Z. has consulted for Cardionovum, CrannMedical, InnovHeart, Meditrial, Opsens Medical, and Replycare. G.W.S. has received speaker or other honoraria from Cook and Infraredx; has served as a consultant to Valfix, TherOx, Robocath, HeartFlow, Ablative Solutions, Vectorious, Miracor, Neovasc, Abiomed, Ancora, Elucid Bio, Occlutech, CorFlow, Apollo Therapeutics, Impulse Dynamics, Reva, Vascular Dynamics, Shockwave, V-Wave, Cardiomech, and Gore; and has equity/options from Ancora, Cagent, Applied Therapeutics, Biostar family of funds, SpectraWave, Orchestra Biomed, Aria, Cardiac Success, Valfix, and MedFocus family of funds.
Figures






References
-
- Ahn JM, Kang SJ, Yoon SH, Park HW, Kang SM, Lee JYet al. Meta-analysis of outcomes after intravascular ultrasound-guided versus angiography-guided drug-eluting stent implantation in 26,503 patients enrolled in three randomized trials and 14 observational studies. Am J Cardiol 2014;113:1338–47. - PubMed
-
- Hu MJ, Tan JS, Yin L, Zhao YY, Gao XJ, Yang JGet al. Clinical outcomes following hemodynamic parameter or intravascular imaging-guided percutaneous coronary intervention in the era of drug-eluting stents: an updated systematic review and Bayesian network meta-analysis of 28 randomized trials and 11,860 patients. Front Cardiovasc Med 2022;9:860189. - PMC - PubMed
-
- Witzenbichler B, Maehara A, Weisz G, Neumann FJ, Rinaldi MJ, Metzger DCet al. Relationship between intravascular ultrasound guidance and clinical outcomes after drug-eluting stents: the assessment of dual antiplatelet therapy with drug-eluting stents (ADAPT-DES) study. Circulation 2014;129:463–70. - PubMed
-
- Soeda T, Uemura S, Park SJ, Jang Y, Lee S, Cho JMet al. Incidence and clinical significance of poststent optical coherence tomography findings: one-year follow-up study from a multicenter registry. Circulation 2015;132:1020–9. - PubMed
-
- Prati F, Di Vito L, Biondi-Zoccai G, Occhipinti M, La Manna A, Tamburino Cet al. Angiography alone versus angiography plus optical coherence tomography to guide decision-making during percutaneous coronary intervention: the Centro per la Lotta contro l'Infarto-Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) study. EuroIntervention 2012;8:823–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
