

Airway and Transpulmonary Driving Pressure by End-Inspiratory Holds During Pressure Support Ventilation
- PMID: 37463722
- PMCID: PMC10589108
- DOI: 10.4187/respcare.10802
Airway and Transpulmonary Driving Pressure by End-Inspiratory Holds During Pressure Support Ventilation
Abstract
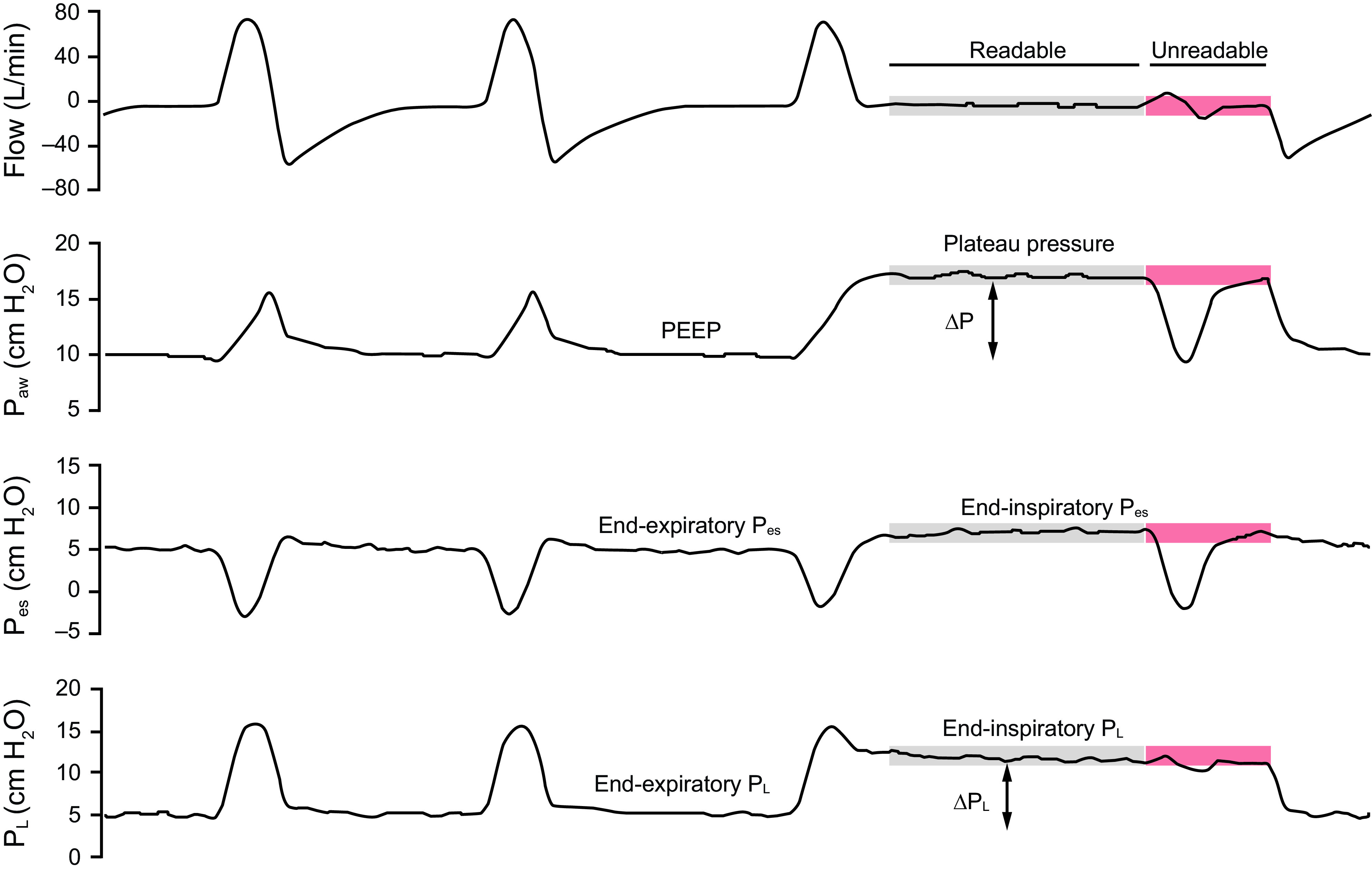
Background: The precision of quasi-static airway driving pressure (ΔP) assessed in pressure support ventilation (PSV) as a surrogate of tidal lung stress is debatable because persistent muscular activity frequently alters the readability of end-inspiratory holds. In this study, we used strict criteria to discard excessive muscular activity during holds and assessed the accuracy of ΔP in predicting global lung stress in PSV. Additionally, we explored whether the physiological effects of high PEEP differed according to the response of respiratory system compliance (CRS).
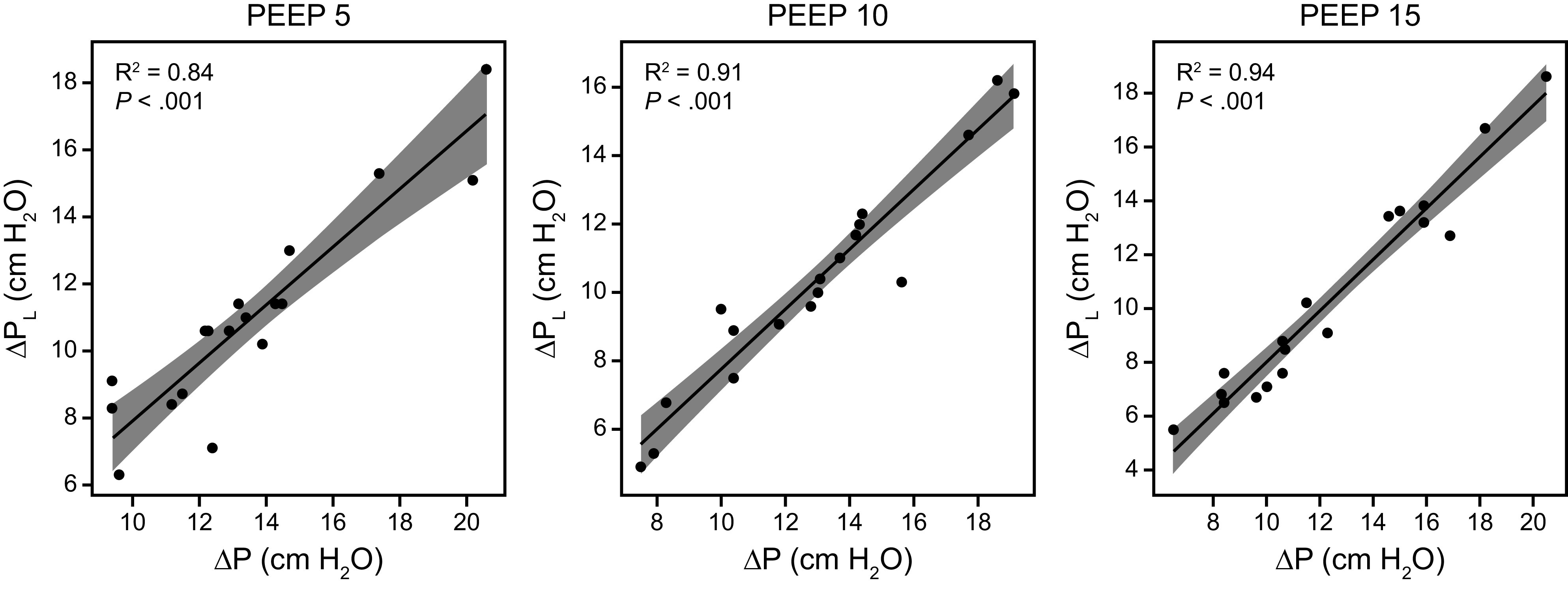
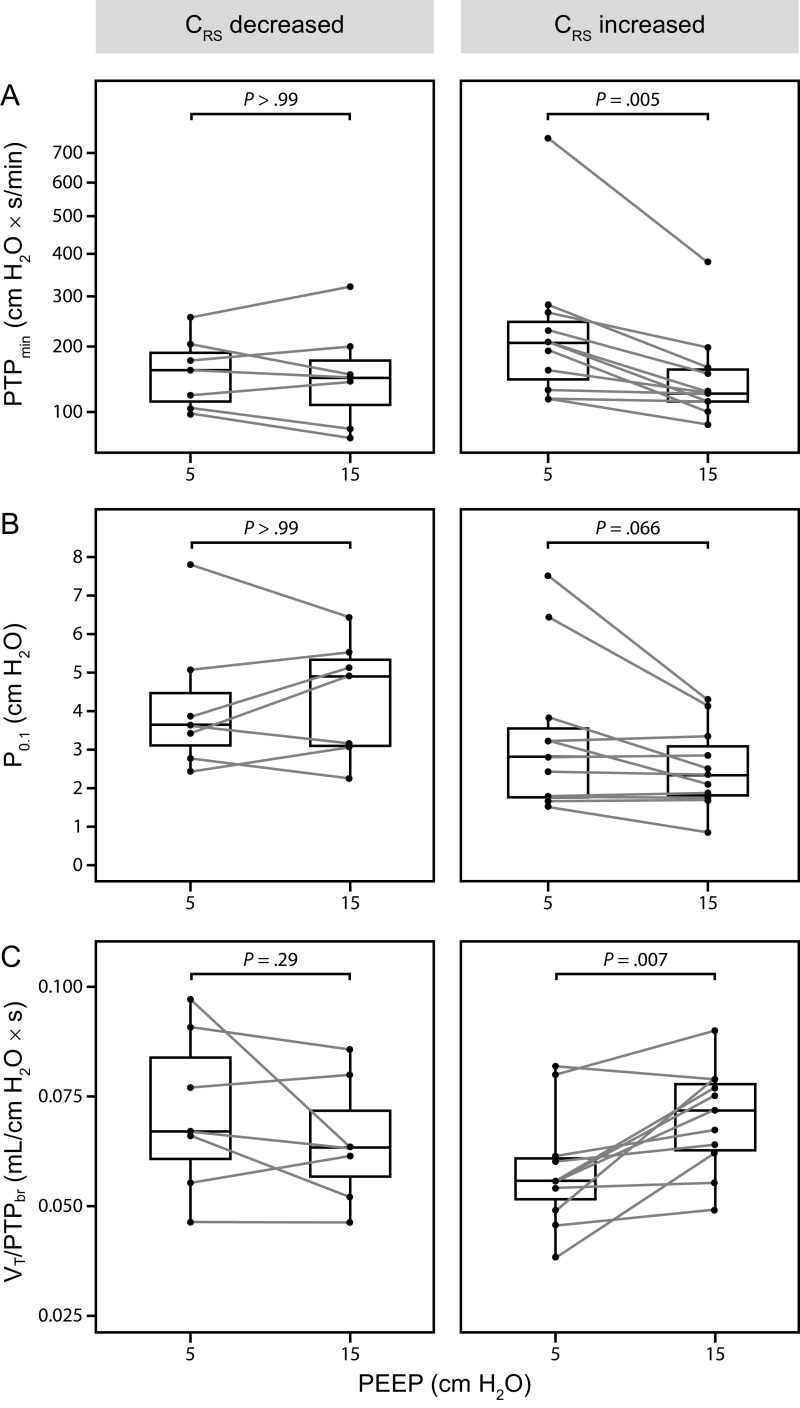
Methods: Adults with ARDS undergoing PSV were enrolled. An esophageal catheter was inserted to calculate lung stress through transpulmonary driving pressure (ΔPL). ΔP and ΔPL were assessed in PSV at PEEP 5, 10, and 15 cm H2O by end-inspiratory holds. CRS was calculated as tidal volume (VT)/ΔP. We analyzed the effects of high PEEP on pressure-time product per minute (PTPmin), airway pressure at 100 ms (P0.1), and VT over PTP per breath (VT/PTPbr) in subjects with increased versus decreased CRS at high PEEP.
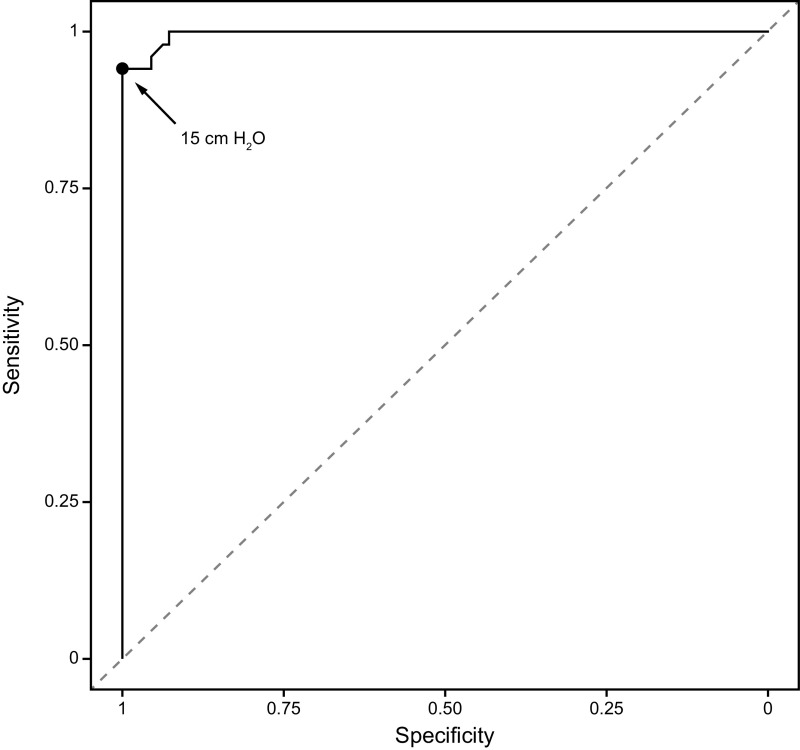
Results: Eighteen subjects and 162 end-inspiratory holds were analyzed; 51/162 (31.5%) of the holds had ΔPL ≥ 12 cm H2O. Significant association between ΔP and ΔPL was found at all PEEP levels (P < .001). ΔP had excellent precision to predict ΔPL, with 15 cm H2O being identified as the best threshold for detecting ΔPL ≥ 12 cm H2O (area under the receiver operating characteristics 0.99 [95% CI 0.98-1.00]). CRS changes from low to high PEEP corresponded well with lung compliance changes (R2 0.91, P < .001) When CRS increased, a significant improvement of PTPmin and VT/PTPbr was found, without changes in P0.1. No benefits were observed when CRS decreased.
Conclusions: In subjects with ARDS undergoing PSV, high ΔP assessed by readable end-inspiratory holds accurately detected potentially dangerous thresholds of ΔPL. Using ΔP to assess changes in CRS induced by PEEP during assisted ventilation may inform whether higher PEEP could be beneficial.
Keywords: acute respiratory distress syndrome; interactive ventilatory support; patient monitoring; respiratory mechanics; ventilator-induced lung injury.
Copyright © 2023 by Daedalus Enterprises.
Conflict of interest statement
Mr Plotnikow discloses relationships with Vapotherm USA and Medtronic Argentina, Panamá, Costa Rica, and México. The remaining authors have disclosed no conflicts of interest.
Figures
References
-
- Protti A, Andreis DT, Monti M, Santini A, Sparacino CC, Langer T, et al. . Lung stress and strain during mechanical ventilation: any difference between statics and dynamics? Crit Care Med 2013;41(4):1046–1055. - PubMed
-
- Chiumello D, Carlesso E, Cadringher P, Caironi P, Valenza F, Polli F, et al. . Lung stress and strain during mechanical ventilation for acute respiratory distress syndrome. Am J Respir Crit Care Med 2008;178(4):346–355. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. ; LUNG SAFE Investigators; ESICM Trials Group. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016;315(8):788–800. - PubMed
-
- Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, et al. . Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med 2015;372(8):747–755. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
