

Patterns of pharmacotherapy for bipolar disorder: A GBC survey
- PMID: 37463846
- PMCID: PMC10794603
- DOI: 10.1111/bdi.13366
Patterns of pharmacotherapy for bipolar disorder: A GBC survey
Abstract
Objectives: To understand treatment practices for bipolar disorders (BD), this study leveraged the Global Bipolar Cohort collaborative network to investigate pharmacotherapeutic treatment patterns in multiple cohorts of well-characterized individuals with BD in North America, Europe, and Australia.
Methods: Data on pharmacotherapy, demographics, diagnostic subtypes, and comorbidities were provided from each participating cohort. Individual site and regional pooled proportional meta-analyses with generalized linear mixed methods were conducted to identify prescription patterns.
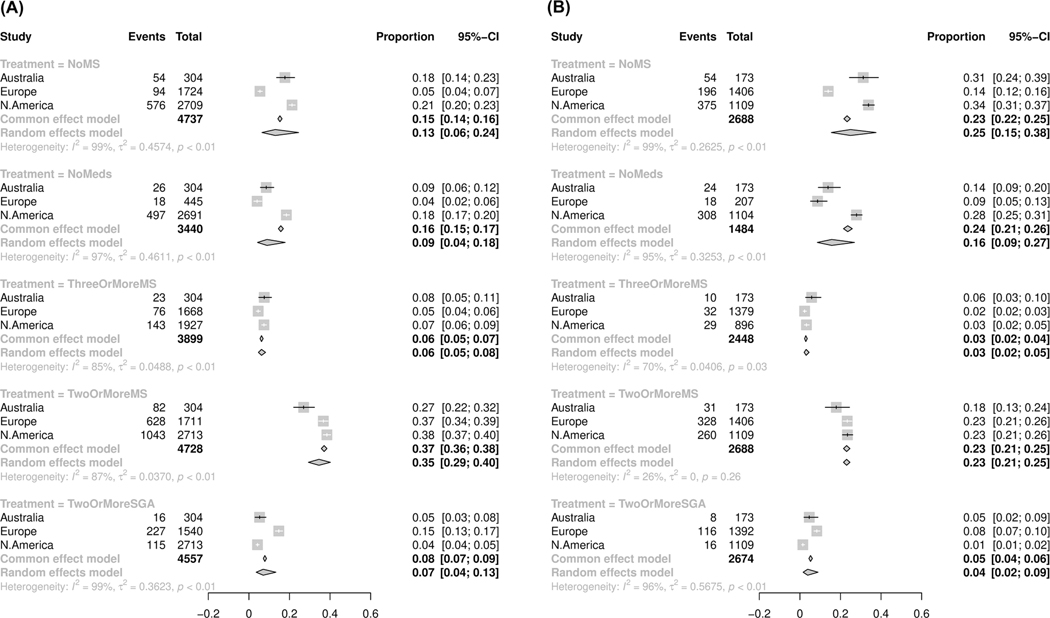
Results: This study included 10,351 individuals from North America (n = 3985), Europe (n = 3822), and Australia (n = 2544). Overall, participants were predominantly female (60%) with BD-I (60%; vs. BD-II = 33%). Cross-sectionally, mood-stabilizing anticonvulsants (44%), second-generation antipsychotics (42%), and antidepressants (38%) were the most prescribed medications. Lithium was prescribed in 29% of patients, primarily in the Australian (31%) and European (36%) cohorts. First-generation antipsychotics were prescribed in 24% of the European versus 1% in the North American cohort. Antidepressant prescription rates were higher in BD-II (47%) compared to BD-I (35%). Major limitations were significant differences among cohorts based on inclusion/exclusion criteria, data source, and time/year of enrollment into cohort.
Conclusions: Mood-stabilizing anticonvulsants, second-generation antipsychotics, and antidepressants were the most prescribed medications suggesting prescription patterns that are not necessarily guideline concordant. Significant differences exist in the prescription practices across different geographic regions, especially the underutilization of lithium in the North American cohorts and the higher utilization of first-generation antipsychotics in the European cohorts. There is a need to conduct future longitudinal studies to further explore these differences and their impact on outcomes, and to inform and implement evidence-based guidelines to help improve treatment practices in BD.
Keywords: antidepressants; antipsychotics; bipolar disorder; lithium; mood stabilizer; pharmacotherapy.
© 2023 The Authors. Bipolar Disorders published by John Wiley & Sons Ltd.
Conflict of interest statement
BS has received research grant support from the Mayo Clinic and the NNDC Momentum grant (unrelated to this study). EV has received grants and served as consultant, advisor, or CME speaker for the following entities: AB-Biotics, AbbVie, Adamed, Angelini, Biogen, Boehringer-Ingelheim, Celon Pharma, Compass, Dainippon Sumitomo Pharma, Ferrer, Gedeon Richter, GH Research, Glaxo-Smith Kline, Janssen, Lundbeck, Medincell, Merck, Novartis, Orion Corporation, Organon, Otsuka, Rovi, Sage, Sanofi-Aventis, Sunovion, Takeda, and Viatris, outside the submitted work. EV’s research was supported by CIBER—Consorcio Centro de Investigación Biomédica en Red—(CB07/09/0004), Instituto de Salud Carlos III, Spanish Ministry of Science and Innovation. EV thanks the support of the Spanish Ministry of Science and Innovation (PI18/00805, PI21/00787) integrated into the Plan Nacional de I + D + I and cofinanced by the ISCIII-Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER), the Instituto de Salud Carlos III, the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2017 SGR 1365), the CERCA Programme, and the Departament de Salut de la Generalitat de Catalunya for the PERIS grant SLT006/17/00357. Thanks to the support of the European Union Horizon 2020 research and innovation program (EU.3.1.1. Understanding health, well-being and disease: Grant No 754907 and EU.3.1.3. Treating and managing disease: Grant No 945151).
NV has received financial support for CME activities and travel funds from the following entities (unrelated to the present work): Angelini, Janssen-Cilag, Lundbeck, Otsuka. GF work is supported by a fellowship from “La Caixa Foundation (ID 100010434 fellowship code LCF/BQ/DR21/11880019). RS has received honoraria from Janssen. AHY has undertaken paid lectures and advisory boards for the following companies with drugs used in affective and related disorders: Astrazenaca, Boehringer Ingelheim, Eli Lilly, LivaNova, Lundbeck, Sunovion, Servier, Livanova, Janssen, Allegan, Bionomics, Sumitomo Dainippon Pharma, COMPASS, Sage, Novartis, and Neurocentrx; is Principal Investigator in the Restore-Life VNS registry study funded by LivaNova; Principal Investigator on ESKETINTRD3004: “An Open-label, Long-term, Safety and Efficacy Study of Intranasal Esketamine in Treatment-resistant Depression”; Principal Investigator on “The Effects of Psilocybin on Cognitive Function in Healthy Participants”; Principal Investigator on “The Safety and Efficacy of Psilocybin in Participants with Treatment-Resistant Depression (P-TRD)”; and UK Chief Investigator for Novartis MDD study MIJ821A12201.
MGM has consulted for Janssen and Otsuka Pharmaceuticals and received research support from Janssen. OAA has received speaker’s honorarium from Sunovion and Lundbeck, and is a consultant to HealthLytix, Norwegian Principal Investigator of CONNEX-1 and MDMA-assistert psykoterapi for behandling av PTSD.
MAF has received research support from Assurex Health, Mayo Foundation, CME/Travel/Honoraria from Carnot Laboratories and American Physician Institute and has Financial Interest/Stock ownership/Royalties in Chymia LLC. The Mayo Clinic Bipolar Biobank was supported by the J. Willard and Alice S. Marriott Foundation. The sponsor did not have a role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
KEB has received grants from Janssen Pharmaceuticals and has received honorarium as an advisory board member for The Bipolar Roadmap Initiative (Milken Institute for Strategic Philanthropy) and Breakthrough Discoveries for thriving with Bipolar Disorder (BD2).
KK has served on the scientific advisory board of AbbVie, and is supported by the Vancouver Coastal Health Research Institute Investigator Award.
LNY has been on speaker/advisory boards for or has received research grants from Alkermes, Allergan, AbbVie, CANMAT, CIHR, Dainippon Sumitomo Pharma, GSK, Intracellular therapies, Lundbeck, Merck, Otsuka, Sanofi, and Sunovion over the past 3 years.
Rest of the authors report no financial relationships with commercial interests.
Figures


References
-
- American Psychiatric Association. Practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(4 Suppl):1–50. - PubMed
-
- Tohen M, Vieta E, Gonzalez-Pinto A, Reed C, Lin D. European mania in bipolar longitudinal evaluation of medication advisory B. Baseline characteristics and outcomes in patients with first episode or multiple episodes of acute mania. J Clin Psychiatry. 2010;71(3):255–261. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
