Clinical effects of Lewy body pathology in cognitively impaired individuals
- PMID: 37464058
- PMCID: PMC10427416
- DOI: 10.1038/s41591-023-02449-7
Clinical effects of Lewy body pathology in cognitively impaired individuals
Abstract
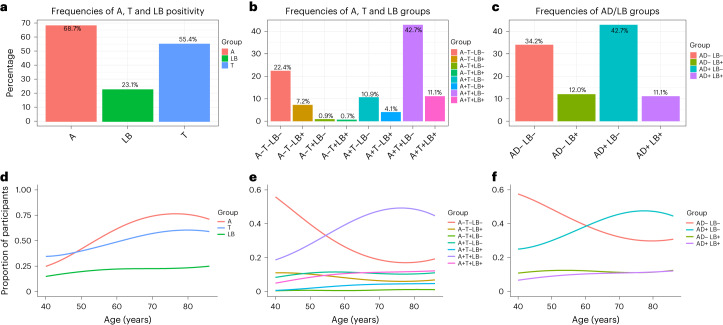
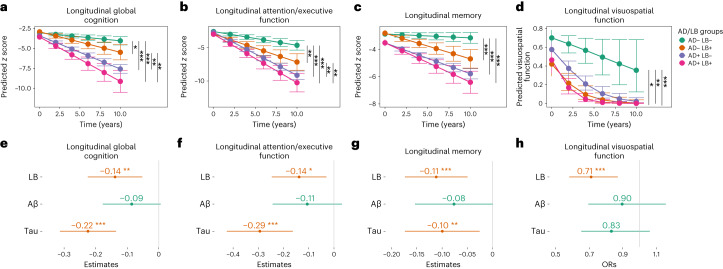
There is poor knowledge about the clinical effects of Lewy body (LB) pathology in patients with cognitive impairment, especially when coexisting with Alzheimer's disease (AD) pathology (amyloid-β and tau). Using a seed amplification assay, we analyzed cerebrospinal fluid for misfolded LB-associated α-synuclein in 883 memory clinic patients with mild cognitive impairment or dementia from the BioFINDER study. Twenty-three percent had LB pathology, of which only 21% fulfilled clinical criteria of Parkinson's disease or dementia with Lewy bodies at baseline. Among these LB-positive patients, 48% had AD pathology. Fifty-four percent had AD pathology in the whole sample (17% of mild cognitive impairment and 24% of patients with dementia were also LB-positive). When examining independent cross-sectional effects, LB pathology but not amyloid-β or tau, was associated with hallucinations and worse attention/executive, visuospatial and motor function. LB pathology was also associated with faster longitudinal decline in all examined cognitive functions, independent of amyloid-β, tau, cognitive stage and a baseline diagnosis of dementia with Lewy bodies/Parkinson's disease. LB status provides a better precision-medicine approach to predict clinical trajectories independent of AD biomarkers and a clinical diagnosis, which could have implications for the clinical management of cognitive impairment and the design of AD and LB drug trials.
© 2023. The Author(s).
Conflict of interest statement
None of the authors has any financial interest in the α-syn SAA test. S.P. has acquired research support (for the institution) from ki elements/Alzheimer Drug Discoveries Foundation. In the past 2 years, he has received consultancy/speaker fees from Bioartic, Biogen, Lilly and Roche. O.H. has acquired research support (for the institution) from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer and Roche. In the past 2 years, he has received consultancy/speaker fees from AC Immune, Amylyx, Alzpath, BioArctic, Biogen, Cerveau, Eisai, Eli Lilly, Fujirebio, Genentech, Merck, Novartis, Novo Nordisk, Roche, Sanofi and Siemens. M.R., S.H., C.Q., N.M.C., S.D., A.M., S.J., S.B., E.S. and P.P. declare no competing interests.
Figures