

Cognitive effects of Lewy body pathology in clinically unimpaired individuals
- PMID: 37464059
- PMCID: PMC10427420
- DOI: 10.1038/s41591-023-02450-0
Cognitive effects of Lewy body pathology in clinically unimpaired individuals
Abstract
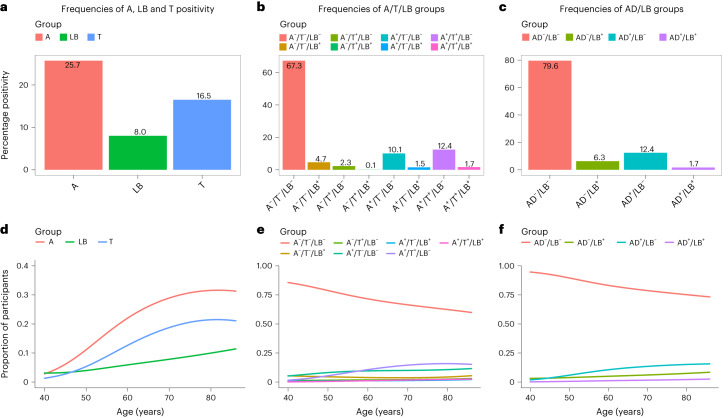
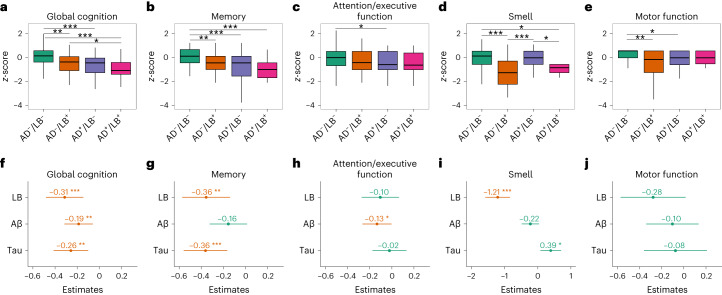
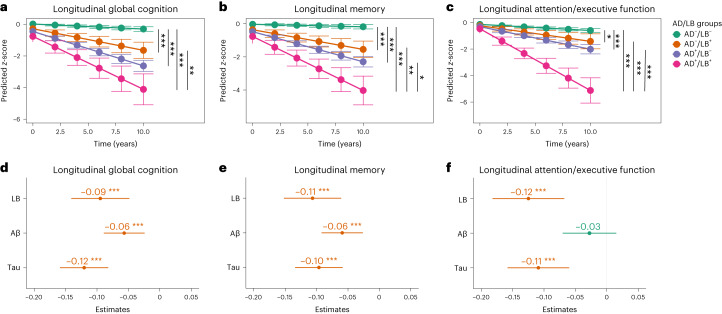
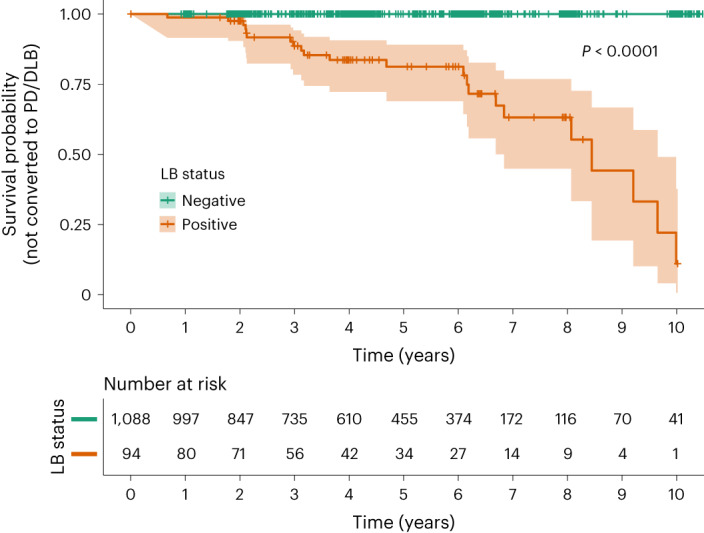
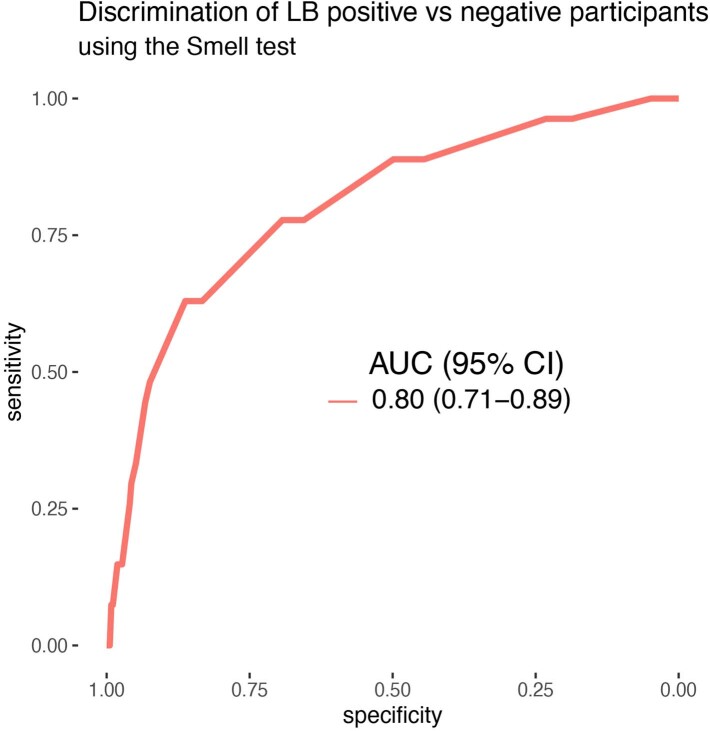
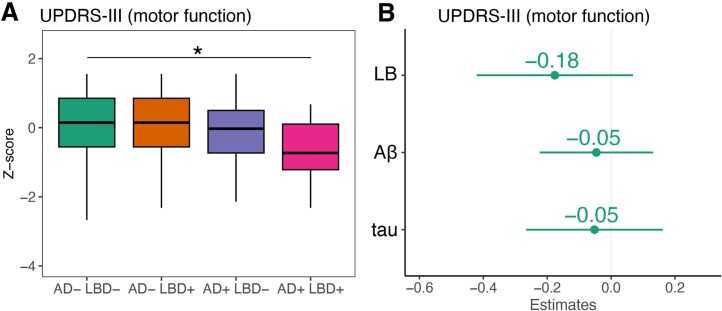
α-Synuclein aggregates constitute the pathology of Lewy body (LB) disease. Little is known about the effects of LB pathology in preclinical (presymptomatic) individuals, either as isolated pathology or coexisting with Alzheimer's disease (AD) pathology (β-amyloid (Aβ) and tau). We examined the effects of LB pathology using a cerebrospinal fluid α-synuclein-seed amplification assay in 1,182 cognitively and neurologically unimpaired participants from the BioFINDER study: 8% were LB positive, 26% Aβ positive (13% of those were LB positive) and 16% tau positive. LB positivity occurred more often in the presence of Aβ positivity but not tau positivity. LB pathology had independently negative effects on cross-sectional and longitudinal global cognition and memory and on longitudinal attention/executive function. Tau had cognitive effects of a similar magnitude, but these were less pronounced for Aβ. Participants with both LB and AD (Aβ and tau) pathology exhibited faster cognitive decline than those with only LB or AD pathology. LB, but not AD, pathology was associated with reduced sense of smell. Only LB-positive participants progressed to clinical LB disease over 10 years. These results are important for individualized prognosis, recruitment and choice of outcome measures in preclinical LB disease trials, but also for the design of early AD trials because >10% of individuals with preclinical AD have coexisting LB pathology.
© 2023. The Author(s).
Conflict of interest statement
None of the authors have any financial interest in the α-syn SAA test. S.P. has acquired research support (for the institution) from ki elements/Alzheimer Drug Discoveries Foundation. In the past 2 years he has received consultancy/speaker fees from Bioartic, Biogen, Eli Lilly and Roche. O.H. has acquired research support (for the institution) from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer and Roche. In the past 2 years he has received consultancy/speaker fees from AC Immune, Amylyx, Alzpath, BioArctic, Biogen, Cerveau, Eisai, Eli Lilly, Fujirebio, Genentech, Novartis, Novo Nordisk, Roche and Siemens. The remaining authors declare no competing interests.
Figures
References
-
- Hansson O. Biomarkers for neurodegenerative diseases. Nat. Med. 2021;27:954–963. - PubMed
-
- Horvath J, Herrmann FR, Burkhard PR, Bouras C, Kovari E. Neuropathology of dementia in a large cohort of patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2013;19:864–868. - PubMed
-
- Klos KJ, et al. Alpha-synuclein pathology in the spinal cords of neurologically asymptomatic aged individuals. Neurology. 2006;66:1100–1102. - PubMed
