

Pain and Opioid Consumption After Laparoscopic Versus Open Gastrectomy for Gastric Cancer: A Secondary Analysis of a Multicenter Randomized Clinical Trial (LOGICA-Trial)
- PMID: 37464143
- PMCID: PMC10579125
- DOI: 10.1007/s11605-023-05728-3
Pain and Opioid Consumption After Laparoscopic Versus Open Gastrectomy for Gastric Cancer: A Secondary Analysis of a Multicenter Randomized Clinical Trial (LOGICA-Trial)
Abstract
Background: Laparoscopic gastrectomy could reduce pain and opioid consumption, compared to open gastrectomy. However, it is difficult to judge the clinical relevance of this reduction, since these outcomes are reported in few randomized trials and in limited detail.
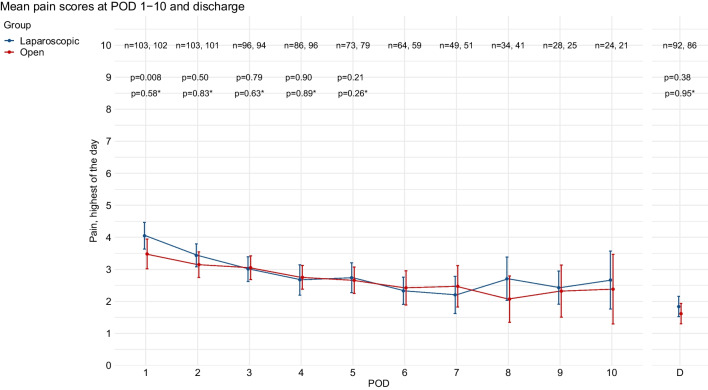
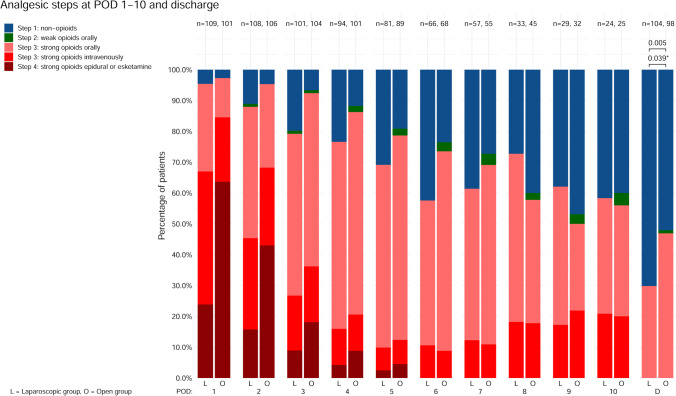
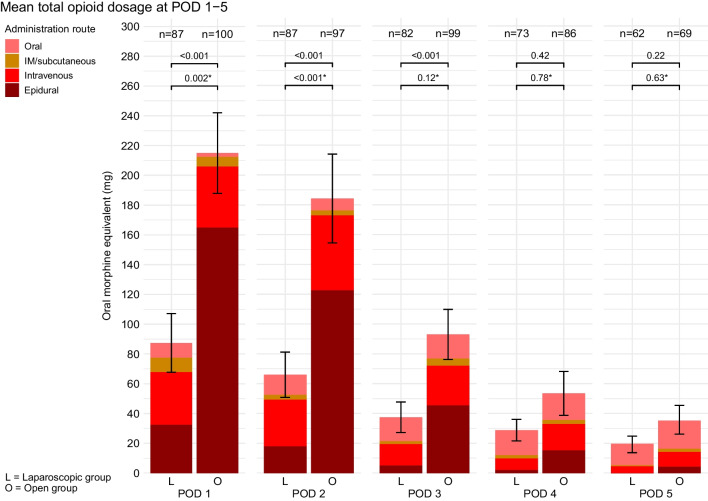
Methods: This secondary analysis of a multicenter randomized trial compared laparoscopic versus open gastrectomy for resectable gastric adenocarcinoma (cT1-4aN0-3bM0). Postoperative pain was analyzed by opioid consumption in oral morphine equivalents (OME, mg/day) at postoperative day (POD) 1-5, WHO analgesic steps, and Numeric Rating Scales (NRS, 0-10) at POD 1-10 and discharge. Regression and mixed model analyses were performed, with and without correction for epidural analgesia.
Results: Between 2015 and 2018, 115 patients in the laparoscopic group and 110 in the open group underwent surgery. Some 16 patients (14%) in the laparoscopic group and 73 patients (66%) in the open group received epidural analgesia. At POD 1-3, mean opioid consumption was 131, 118, and 53 mg OME lower in the laparoscopic group, compared to the open group, respectively (all p < 0.001). After correcting for epidural analgesia, these differences remained significant at POD 1-2 (47 mg OME, p = 0.002 and 69 mg OME, p < 0.001, respectively). At discharge, 27% of patients in the laparoscopic group and 43% patients in the open group used oral opioids (p = 0.006). Mean highest daily pain scores were between 2 and 4 at all PODs, < 2 at discharge, and did not relevantly differ between treatment arms.
Conclusion: In this multicenter randomized trial, postoperative pain was comparable between laparoscopic and open gastrectomy. After laparoscopic gastrectomy, this was generally achieved without epidural analgesia and with fewer opioids.
Trial registration: NCT02248519.
Keywords: Gastrectomy; Gastric cancer; Laparoscopic gastrectomy; Opioid consumption; Pain; Randomized trial; Surgery.
© 2023. The Author(s).
Conflict of interest statement
Misha D. P. Luyer
Consulting or Advisory Role: Galvani, Medtronic.
Research Funding: Dutch Cancer Foundation.
Travel, Accommodations, Expenses: Medtronic.
Grard A. P. Nieuwenhuijzen
Consulting or Advisory Role: Medtronic.
Research Funding: Medtronic.
Jelle P. Ruurda
Consulting or Advisory Role: Intuitive Surgical.
Richard van Hillegersberg
Consulting or Advisory Role: Intuitive Surgical, Medtronic.
No other potential conflicts of interest were reported.
Figures
References
-
- Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4) The Lancet. 2019;6736(18):1–10. - PubMed
-
- Brenkman HJF, Ruurda JP, Verhoeven RHA, van Hillegersberg R. Safety and feasibility of minimally invasive gastrectomy during the early introduction in the Netherlands: short-term oncological outcomes comparable to open gastrectomy. Gastric Cancer. 2017;20(5):853–860. doi: 10.1007/s10120-017-0695-8. - DOI - PMC - PubMed
-
- Gertsen EC, Brenkman HJF, Haverkamp L, Read M, Ruurda JP, Van Hillegersberg R. Worldwide Practice in Gastric Cancer Surgery: A 6-Year Update. Dig Surg. 2021; - PubMed
-
- Dutch Upper GI Cancer Audit (DUCA) annual report 2019 [Internet]. [cited 2021 Aug 24]. Available from: https://dica.nl/jaarrapportage-2019/duca
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
