

Failure of diltiazem to prevent 1:1 conduction of atrial flutter: a case report
- PMID: 37464369
- PMCID: PMC10355050
- DOI: 10.1186/s13256-023-03947-5
Failure of diltiazem to prevent 1:1 conduction of atrial flutter: a case report
Abstract
Background: Atrial flutter with 1:1 conduction to the ventricles is a dangerous cardiac arrhythmia. Contemporary guidelines recommend atrioventricular nodal blocking agents should be co-administered with class 1C anti-arrhythmics, as prophylaxis against 1:1 flutter. No guidance is provided on the type or strength of atrioventricular nodal blockade required, and in practice, these agents are frequently prescribed at low dose, or even omitted, due to their side effect profile.
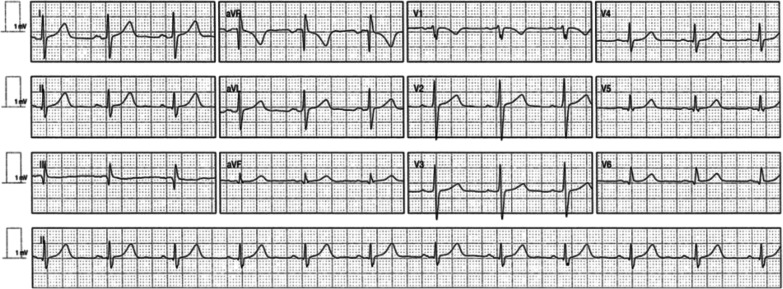
Case presentation: A 62 year old Caucasian man with a history of paroxysmal atrial fibrillation treated with flecainide, presented with atrial flutter with 1:1 conduction to the ventricles and was cardioverted. Diltiazem was added to prevent this complication and he again presented with atrial flutter with 1:1 conduction to the ventricles, despite prophylaxis with coadministration of diltiazem.
Conclusions: This case report demonstrates failure of diltiazem to prevent 1:1 flutter in a patient chronically treated with flecainide for paroxysmal atrial fibrillation.
Keywords: 1:1 conduction; Atrial flutter; Case report; Class 1c; Diltiazem; Flecainide.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Management of paroxysmal atrial flutter that occurred in an outpatient prior to dental surgery: a case report.BMC Oral Health. 2019 Dec 4;19(1):271. doi: 10.1186/s12903-019-0963-6. BMC Oral Health. 2019. PMID: 31801491 Free PMC article.
-
Flecainide-Induced Atrial Flutter With 1:1 Conduction Complicated by Ventricular Fibrillation After Electrical Cardioversion.Tex Heart Inst J. 2021 Jun 4;48(2):e197099. doi: 10.14503/THIJ-19-7099. Tex Heart Inst J. 2021. PMID: 34086956 Free PMC article.
-
1:1 atrial flutter induced by flecainide, whilst the patient was at rest.Am J Emerg Med. 2018 Nov;36(11):2131.e3-2131.e5. doi: 10.1016/j.ajem.2018.07.040. Epub 2018 Jul 18. Am J Emerg Med. 2018. PMID: 30033133
-
[Pharmacology of modern anti-arrhythmia drugs in therapy of supraventricular tachycardia].Z Gesamte Inn Med. 1993 Sep;48(9):425-9. Z Gesamte Inn Med. 1993. PMID: 8212747 Review. German.
-
[Supraventricular tachycardia with wide QRS complexes during Vaughan-Williams class I anti-arrhythmic treatment. Diagnostic and therapeutic implications].Arch Mal Coeur Vaiss. 1995 Dec;88(12):1869-74. Arch Mal Coeur Vaiss. 1995. PMID: 8729368 Review. French.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
