

Efficacy of interactive manual dexterity training after stroke: a pilot single-blinded randomized controlled trial
- PMID: 37464404
- PMCID: PMC10355015
- DOI: 10.1186/s12984-023-01213-9
Efficacy of interactive manual dexterity training after stroke: a pilot single-blinded randomized controlled trial
Abstract
Objective: To compare the efficacy of Dextrain Manipulandum™ training of dexterity components such as force control and independent finger movements, to dose-matched conventional therapy (CT) post-stroke.
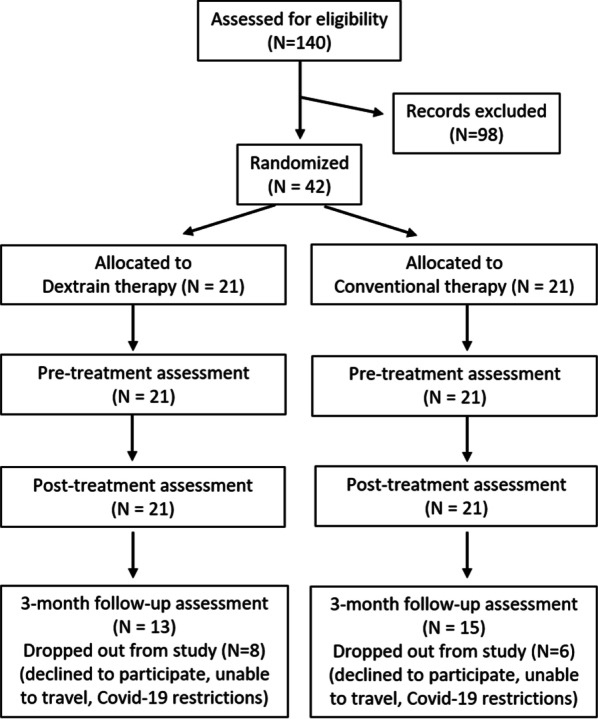
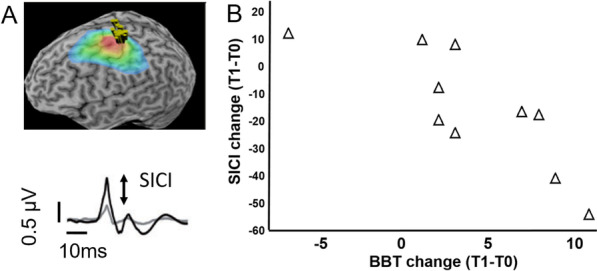
Methods: A prospective, single-blind, pilot randomized clinical trial was conducted. Chronic-phase post-stroke patients with mild-to-moderate dexterity impairment (Box and Block Test (BBT) > 1) received 12 sessions of Dextrain or CT. Blinded measures were obtained before and after training and at 3-months follow-up. Primary outcome was BBT-change (after-before training). Secondary outcomes included changes in motor impairments, activity limitations and dexterity components. Corticospinal excitability and short intracortical inhibition (SICI) were measured using transcranial magnetic stimulation.
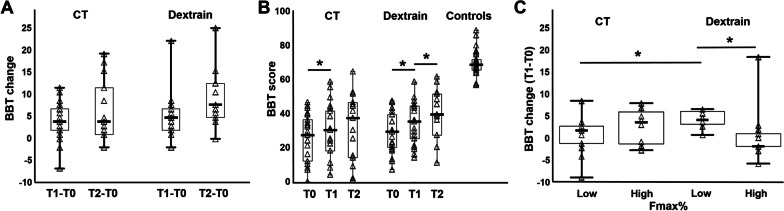
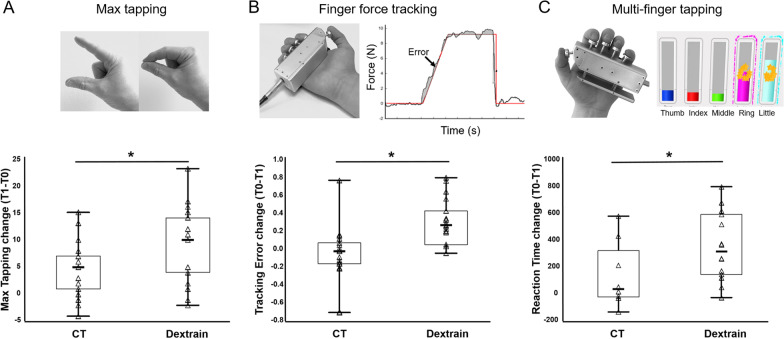
Results: BBT-change after training did not differ between the Dextrain (N = 21) vs CT group (N = 21) (median [IQR] = 5[2-7] vs 4[2-7], respectively; P = 0.36). Gains in BBT were maintained at the 3-month post-training follow-up, with a non-significant trend for enhanced BBT-change in the Dextrain group (median [IQR] = 3[- 1-7.0], P = 0.06). Several secondary outcomes showed significantly larger changes in the Dextrain group: finger tracking precision (mean ± SD = 0.3 ± 0.3N vs - 0.1 ± 0.33N; P < 0.0018), independent finger movements (34.7 ± 25.1 ms vs 7.7 ± 18.5 ms, P = 0.02) and maximal finger tapping speed (8.4 ± 7.1 vs 4.5 ± 4.9, P = 0.045). At follow-up, Dextrain group showed significantly greater improvement in Motor Activity Log (median/IQR = 0.7/0.2-0.8 vs 0.2/0.1-0.6, P = 0.05). Across both groups SICI increased in patients with greater BBT-change (Rho = 0.80, P = 0.006). Comparing Dextrain subgroups with maximal grip force higher/lower than median (61.2%), BBT-change was significantly larger in patients with low vs high grip force (7.5 ± 5.6 vs 2.9 ± 2.8; respectively, P = 0.015).
Conclusions: Although immediate improvements in gross dexterity post-stroke did not significantly differ between Dextrain training and CT, our findings suggest that Dextrain enhances recovery of several dexterity components and reported hand-use, particularly when motor impairment is moderate (low initial grip force). Findings need to be confirmed in a larger trial. Trial registration ClinicalTrials.gov NCT03934073 (retrospectively registered).
Keywords: Dexterity; Finger training; Hand use; RCT; Stroke; Upper limb.
© 2023. The Author(s).
Conflict of interest statement
MT, MAM and PGL have patented the method for multidimensional measurement of manual dexterity (WO2016184935A3). MT and PGL are founding members of start-up company Dextrain (started in 2021) who owns the commercial rights. MT now works for the start-up full-time. PGL, head of the scientific board, reports no financial gain in advising the company. CR is a member of the scientific board of the company but receives no financial benefits. The other authors report no financial interests or potential conflicts of interest.
Figures
References
-
- Kwakkel G, Kollen BJ, van der Grond J, Prevo AJ. Probability of regaining dexterity in the flaccid upper limb: impact of severity of paresis and time since onset in acute stroke. Stroke. 2003;34(9):2181–2186. doi: 10.1161/01.STR.0000087172.16305.CD. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
