

Intravascular imaging during percutaneous coronary intervention: temporal trends and clinical outcomes in the USA
- PMID: 37464975
- PMCID: PMC10567999
- DOI: 10.1093/eurheartj/ehad430
Intravascular imaging during percutaneous coronary intervention: temporal trends and clinical outcomes in the USA
Abstract
Aims: Prior trials have demonstrated that intravascular imaging (IVI)-guided percutaneous coronary intervention (PCI) results in less frequent target lesion revascularization and major adverse cardiovascular events (MACEs) compared with standard angiographic guidance. The uptake and associated outcomes of IVI-guided PCI in contemporary clinical practice in the USA remain unclear. Accordingly, temporal trends and comparative outcomes of IVI-guided PCI relative to PCI with angiographic guidance alone were examined in a broad, unselected population of Medicare beneficiaries.
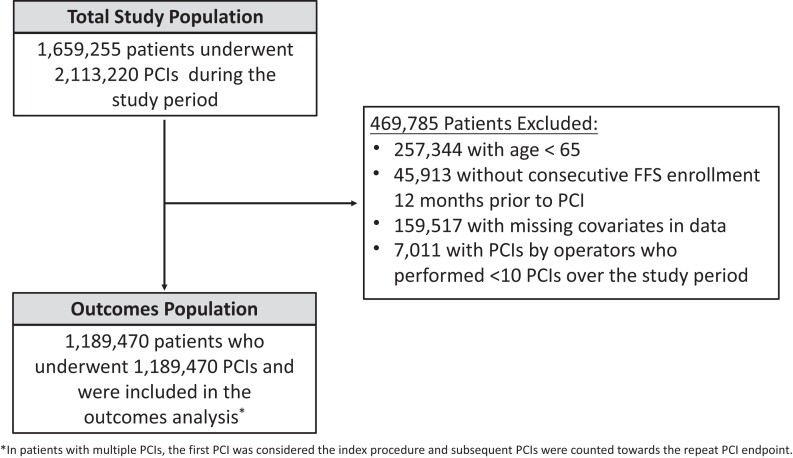
Methods and results: Retrospective cohort study of Medicare beneficiary data from 1 January 2013, through 31 December 2019 to evaluate temporal trends and comparative outcomes of IVI-guided PCI as compared with PCI with angiography guidance alone in both the inpatient and outpatient settings. The primary outcomes were 1 year mortality and MACE, defined as the composite of death, myocardial infarction (MI), repeat PCI, or coronary artery bypass graft surgery. Secondary outcomes were MI or repeat PCI at 1 year. Multivariable Cox regression was used to estimate the adjusted association between IVI guidance and outcomes. Falsification endpoints (hospitalized pneumonia and hip fracture) were used to assess for potential unmeasured confounding. The study population included 1 189 470 patients undergoing PCI (38.0% female, 89.8% White, 65.1% with MI). Overall, IVI was used in 10.5% of the PCIs, increasing from 9.5% in 2013% to 15.4% in 2019. Operator IVI use was variable, with the median operator use of IVI 3.92% (interquartile range 0.36%-12.82%). IVI use during PCI was associated with lower adjusted rates of 1 year mortality [adjusted hazard ratio (aHR) 0.96, 95% confidence interval (CI) 0.94-0.98], MI (aHR 0.97, 95% CI 0.95-0.99), repeat PCI (aHR 0.74, 95% CI 0.73-0.75), and MACE (aHR 0.85, 95% CI 0.84-0.86). There was no association with the falsification endpoint of hospitalized pneumonia (aHR 1.02, 95% CI 0.99-1.04) or hip fracture (aHR 1.02, 95% CI 0.94-1.10).
Conclusion: Among Medicare beneficiaries undergoing PCI, use of IVI has increased over the previous decade but remains relatively infrequent. IVI-guided PCI was associated with lower risk-adjusted mortality, acute MI, repeat PCI, and MACE.
Keywords: Intravascular imaging; Intravascular ultrasound; Optical coherence tomography; Percutaneous coronary intervention.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures





Comment in
-
Intravascular imaging: a glass half empty or half full?Eur Heart J. 2023 Oct 12;44(38):3856-3858. doi: 10.1093/eurheartj/ehad573. Eur Heart J. 2023. PMID: 37667652 No abstract available.
-
Challenge of Measuring Outcomes For Intravascular Imaging During Percutaneous Coronary Intervention from Administrative Database.Am J Cardiol. 2024 Feb 1;212:143. doi: 10.1016/j.amjcard.2023.11.059. Epub 2023 Nov 30. Am J Cardiol. 2024. PMID: 38042268 No abstract available.
Similar articles
-
Intravascular Imaging Improves Clinical Outcomes of Percutaneous Coronary Intervention for Chronic Total Occlusions: A Meta-Analysis of Randomized Controlled Trials.Am J Cardiol. 2025 Jun 15;245:62-70. doi: 10.1016/j.amjcard.2025.03.011. Epub 2025 Mar 11. Am J Cardiol. 2025. PMID: 40081612
-
Intravascular imaging-guided versus angiography-guided percutaneous coronary intervention in patients with diabetes mellitus: Rationale and design of an international, multicenter, randomized IVI-DIABETES trial.Am Heart J. 2025 May;283:81-88. doi: 10.1016/j.ahj.2025.01.017. Epub 2025 Feb 4. Am Heart J. 2025. PMID: 39914556
-
Intravascular imaging-guided vs. angiography-guided percutaneous coronary intervention: A systematic review and meta-analysis of randomized controlled trials in high-risk patients and complex coronary anatomies.Int J Cardiol. 2024 Dec 1;416:132510. doi: 10.1016/j.ijcard.2024.132510. Epub 2024 Aug 31. Int J Cardiol. 2024. PMID: 39222885
-
Intravascular imaging-guided percutaneous coronary intervention for heavily calcified coronary lesions: a systematic review and meta-analysis.Int J Cardiovasc Imaging. 2024 Aug;40(8):1653-1659. doi: 10.1007/s10554-024-03150-7. Epub 2024 Jun 14. Int J Cardiovasc Imaging. 2024. PMID: 38874673
-
Long-Term Outcomes of Coronary Stenting With and Without Use of Intravascular Ultrasound.JACC Cardiovasc Interv. 2020 Aug 24;13(16):1880-1890. doi: 10.1016/j.jcin.2020.04.052. JACC Cardiovasc Interv. 2020. PMID: 32819477 Free PMC article.
Cited by
-
CVIT 2025 clinical expert consensus document on intravascular ultrasound.Cardiovasc Interv Ther. 2025 Apr;40(2):211-225. doi: 10.1007/s12928-025-01090-0. Epub 2025 Jan 27. Cardiovasc Interv Ther. 2025. PMID: 39870989 Free PMC article. Review.
-
Comprehensive full-vessel segmentation and volumetric plaque quantification for intracoronary optical coherence tomography using deep learning.Eur Heart J Digit Health. 2025 Mar 15;6(3):404-416. doi: 10.1093/ehjdh/ztaf021. eCollection 2025 May. Eur Heart J Digit Health. 2025. PMID: 40395415 Free PMC article.
-
Intravascular Coronary Imaging Update: Advances, Clinical Applications, and Future Directions.Curr Cardiol Rep. 2025 Jul 11;27(1):111. doi: 10.1007/s11886-025-02243-6. Curr Cardiol Rep. 2025. PMID: 40646403 Free PMC article. Review.
-
Deep-learning-driven optical coherence tomography analysis for cardiovascular outcome prediction in patients with acute coronary syndrome.Eur Heart J Digit Health. 2024 Sep 27;5(6):692-701. doi: 10.1093/ehjdh/ztae067. eCollection 2024 Nov. Eur Heart J Digit Health. 2024. PMID: 39563910 Free PMC article.
-
Quantitative Coronary Angiography Guidance for Drug-Eluting Stent Implantation: A Narrative Review.Health Sci Rep. 2024 Dec 17;7(12):e70286. doi: 10.1002/hsr2.70286. eCollection 2024 Dec. Health Sci Rep. 2024. PMID: 39691560 Free PMC article.
References
-
- Darmoch F, Alraies MC, Al-Khadra Y, Moussa Pacha H, Pinto DS, Osborn EA. Intravascular ultrasound imaging-guided versus coronary angiography-guided percutaneous coronary intervention: a systematic review and meta-analysis. J Am Heart Assoc 2020;9:e013678. 10.1161/JAHA.119.013678 - DOI - PMC - PubMed
-
- Buccheri S, Franchina G, Romano S, Puglisi S, Venuti G, D’Arrigo P, et al. . Clinical outcomes following intravascular imaging-guided versus coronary angiography–guided percutaneous coronary intervention with stent implantation: a systematic review and Bayesian network meta-analysis of 31 studies and 17,882 patients. JACC Cardiovasc Interv 2017;10:2488–98. 10.1016/j.jcin.2017.08.051 - DOI - PubMed
-
- Yeh RW, Kennedy K, Spertus JA, Parikh SA, Sakhuja R, Anderson HV, et al. . Do postmarketing surveillance studies represent real-world populations? A comparison of patient characteristics and outcomes after carotid artery stenting. Circulation 2011;123:1384–90. 10.1161/CIRCULATIONAHA.110.991075 - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
