

Pediatric Seizure Team-based Learning
- PMID: 37465215
- PMCID: PMC10332555
- DOI: 10.21980/J8MD22
Pediatric Seizure Team-based Learning
Abstract
Audience: The target audiences for this team-based learning are emergency medicine and emergency medicine-pediatric resident physicians.
Introduction/background: Pediatric seizure is a common presenting complaint in the emergency department. It is said that over 470,000 children have a diagnosed seizure disorder1 and 2%-5% of children aged 6 months to five years will have a febrile seizure at some point during childhood.2 While there are many published educational materials related to pediatric seizure, they are simulation-based, and/or isolated to management of one underlying diagnosis.3,4,5,6 Therefore, this team-based learning uses four cases to provide an understanding of the possible causes of seizure in children, as well as the management, workup, and disposition for emergency medicine residents in training.
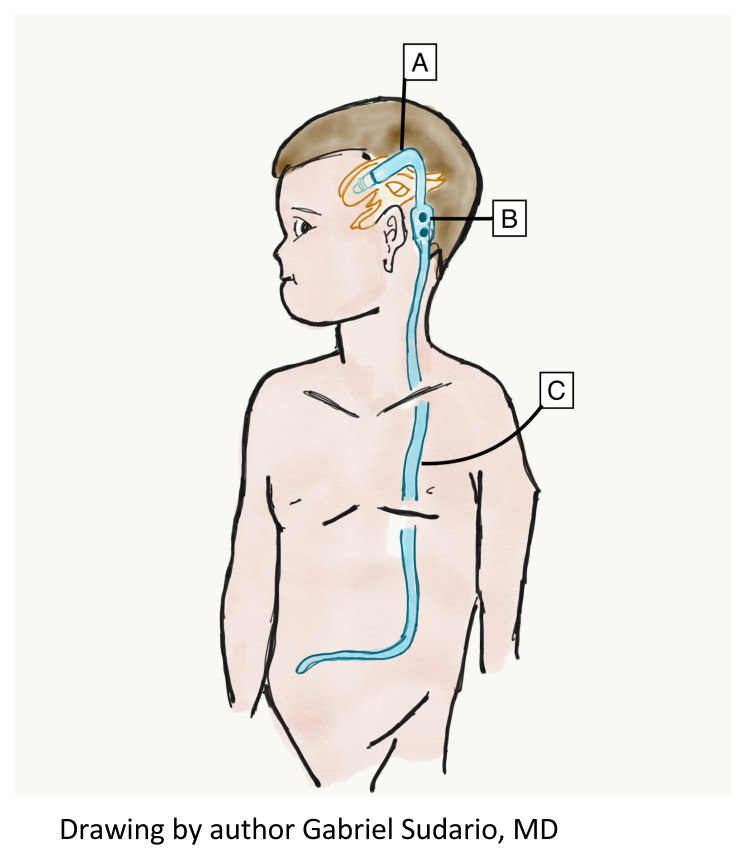
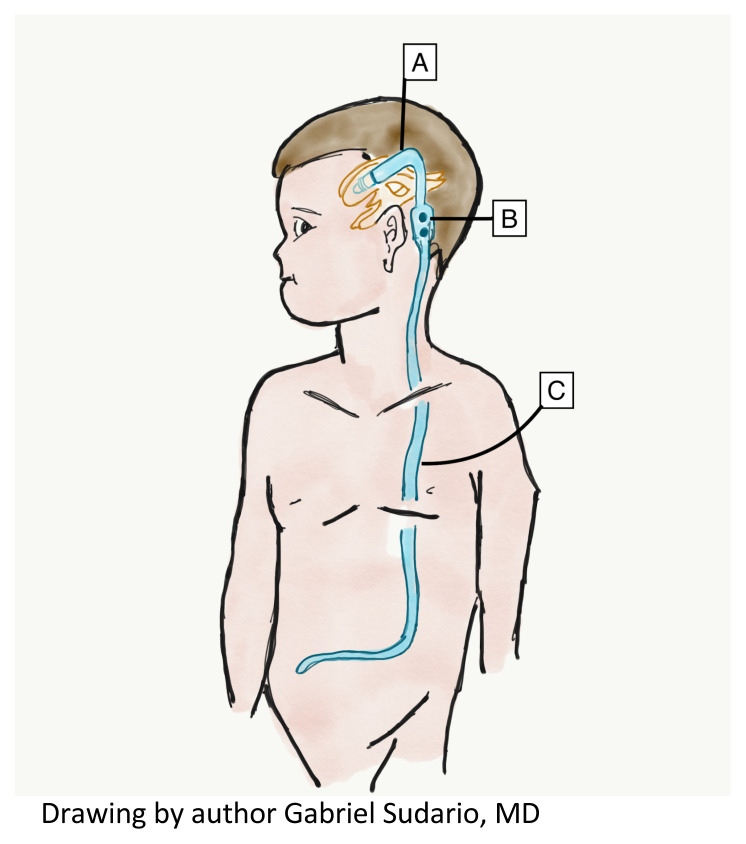
Educational objectives: By the end of this TBL session, learners should be able to:Define features of simple versus complex febrile seizureDiscuss which patients with seizure may require further diagnostic workupSummarize a discharge discussion for a patient with simple febrile seizuresIdentify a differential diagnosis for pediatric patients presenting with seizureDefine features of status epilepticusReview an algorithm for the pharmacologic management of status epilepticusIndicate medication dosing and routes of various benzodiazepine treatmentsObtain a thorough history in an infant patient with seizures to recognize hyponatremia due to improperly prepared formulaChoose the appropriate treatment for a patient with a hyponatremic seizureDescribe the anatomy of a ventriculoperitoneal (VP) shuntRelate a differential diagnosis of VP shunt malfunctionCompare and contrast the neuroimaging options for a patient with a VP shunt.
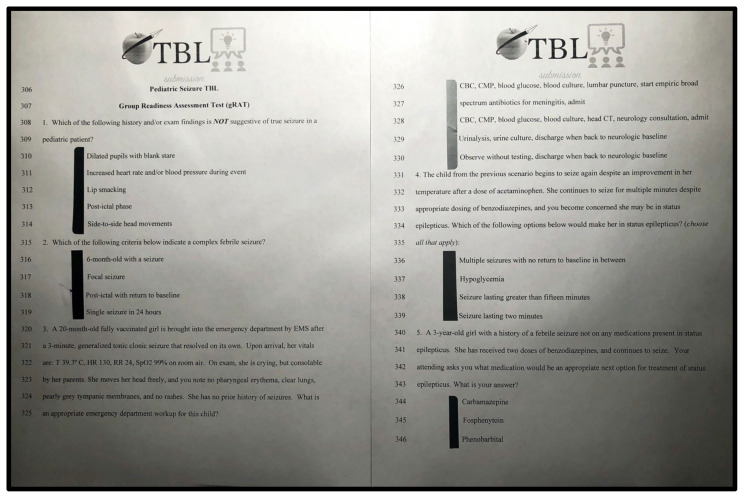
Educational methods: This team-based learning is a classic TBL because it contains learner responsible content (LRC), an individual readiness assessment test (iRAT), a multiple-choice group RAT (gRAT) with immediate feedback assessment technique (IF/AT), and a group application exercise (GAE).
Research methods: We received formative feedback through conversations with learners afterwards, who stated they enjoyed the activity and felt it was highly useful for their learning; in addition, instructors discussed after the session and made changes accordingly.
Results: We collected verbal feedback from instructors and learners after the session. Learners and instructors felt that it was very successful with limited modifications, in particular, the need for more time to complete the activity. Therefore, we suggest a 90 minute rather than 60-minute timeframe to adequately cover all material.
Discussion: Pediatric seizure is a common complaint in the emergency department. It can be a difficult subject for the emergency medicine resident to master based on the variety of presentations. Indeed, the cause, management, and disposition may vary greatly; the etiology may range from benign to life-threatening, sometimes requiring minimal and at other times an extensive workup, with an ultimate disposition of either discharge home or admission to a pediatric intensive care unit. Therefore, team-based learning is well-suited to work through some of the complexities of such cases, and we found this educational session to be highly effective.
Topics: Pediatric seizure, simple febrile seizure, complex febrile seizure, status epilepticus, hyponatremic seizure, ventriculoperitoneal (VP) shunt, team-based learning.
© 2020 Paradise Dimeo, et al.
Figures
Similar articles
-
Hypertensive Emergency Team-Based Learning.J Educ Teach Emerg Med. 2024 Apr 30;9(2):T1-T39. doi: 10.21980/J8BP90. eCollection 2024 Apr. J Educ Teach Emerg Med. 2024. PMID: 38707946 Free PMC article.
-
Febrile Seizure Team-based Learning.J Educ Teach Emerg Med. 2020 Oct 15;5(4):T45-T68. doi: 10.21980/J8JD12. eCollection 2020 Oct. J Educ Teach Emerg Med. 2020. PMID: 37465331 Free PMC article.
-
The Suicidal Patient in the Emergency Department Team-Based Learning Activity.J Educ Teach Emerg Med. 2023 Jan 31;8(1):T1-T37. doi: 10.21980/J8892X. eCollection 2023 Jan. J Educ Teach Emerg Med. 2023. PMID: 37465036 Free PMC article.
-
Vomiting in Pediatric Patients.J Educ Teach Emerg Med. 2020 Oct 15;5(4):T1-T44. doi: 10.21980/J8P363. eCollection 2020 Oct. J Educ Teach Emerg Med. 2020. PMID: 37465339 Free PMC article.
-
Little Patients, Big Tasks - A Pediatric Emergency Medicine Escape Room.J Educ Teach Emerg Med. 2023 Oct 31;8(4):SG1-SG19. doi: 10.21980/J89W70. eCollection 2023 Oct. J Educ Teach Emerg Med. 2023. PMID: 37969155 Free PMC article.
References
-
- Zack MM, Kobau R. National and state estimates of the numbers of adults and children with active epilepsy — United States. Center for Disease Control and Prevention; 2015. [Accessed January 15, 2019]. http://www.cdc.gov/mmwr/volumes/66/wr/mm6631a1.htm . - PMC - PubMed
-
- Van der Berg BJ, Yerushalmy J. Studies on convulsive disorders in young children. I. Incidence of febrile and nonfebrile convulsions by age and other factors. Pediatr Res. 1969;3(4):298–304. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous