

Managing the cancer backlog: a national population-based study of patient mobility, waiting times and 'spare capacity' for cancer surgery
- PMID: 37465324
- PMCID: PMC10350851
- DOI: 10.1016/j.lanepe.2023.100642
Managing the cancer backlog: a national population-based study of patient mobility, waiting times and 'spare capacity' for cancer surgery
Abstract
Background: Waiting times for cancer treatments continue to increase in many countries. In this study we estimated potential 'spare surgical capacity' in the English NHS and identified regions more likely to have spare capacity based on patterns of patient mobility (the extent to which patients receive surgery at hospitals other than their nearest).
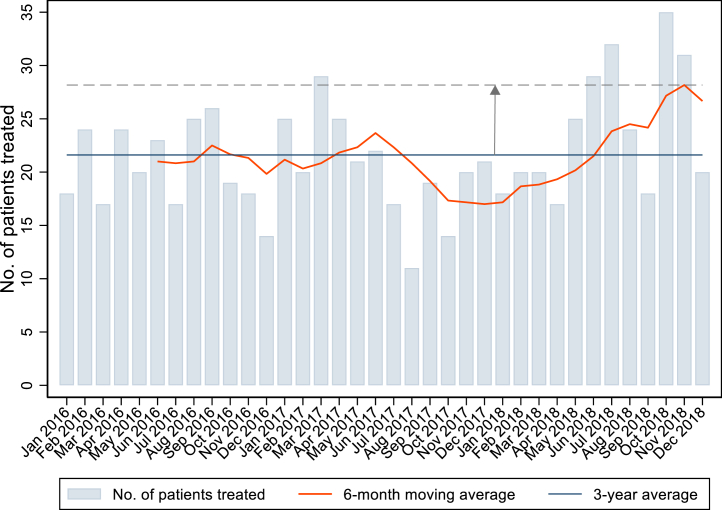
Methods: We identified patients who had an elective breast or colorectal cancer surgical resection between January 2016 and December 2018. We estimated each hospital's 'maximum surgical capacity' as the maximum 6-month moving average of its surgical volume. 'Spare surgical capacity' was estimated as the difference between maximum surgical capacity and observed surgical volume. We assessed the association between spare surgical capacity and whether a hospital performed more or fewer procedures than expected due to patient mobility as well as the association between spare surgical capacity and whether or not waiting times targets for treatment were likely to be met.
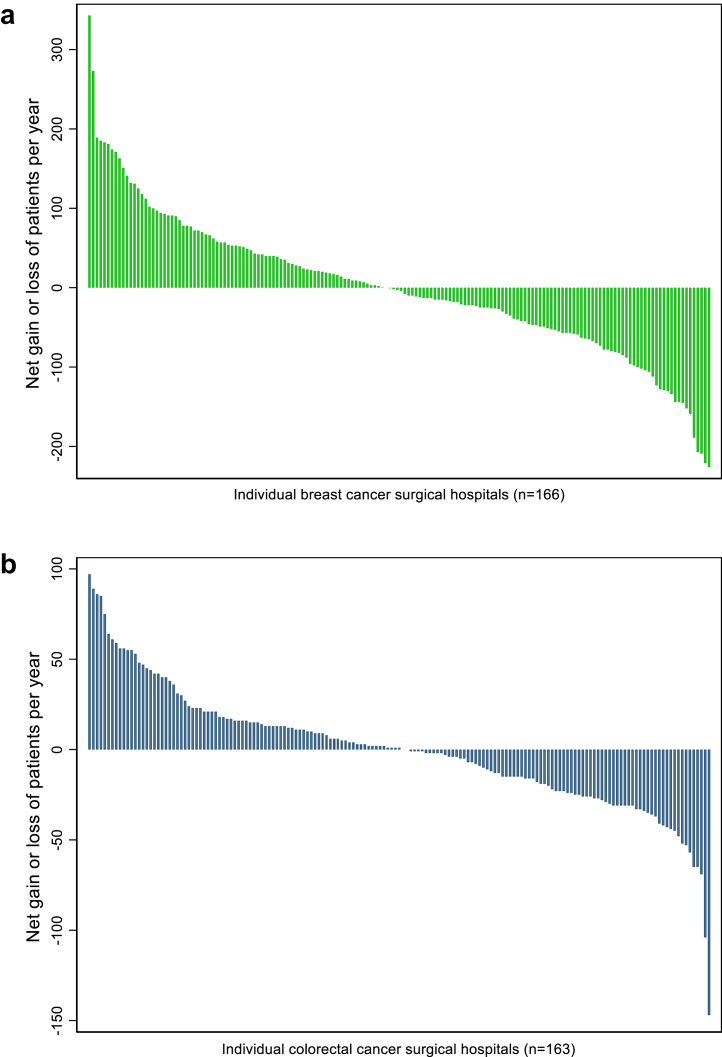
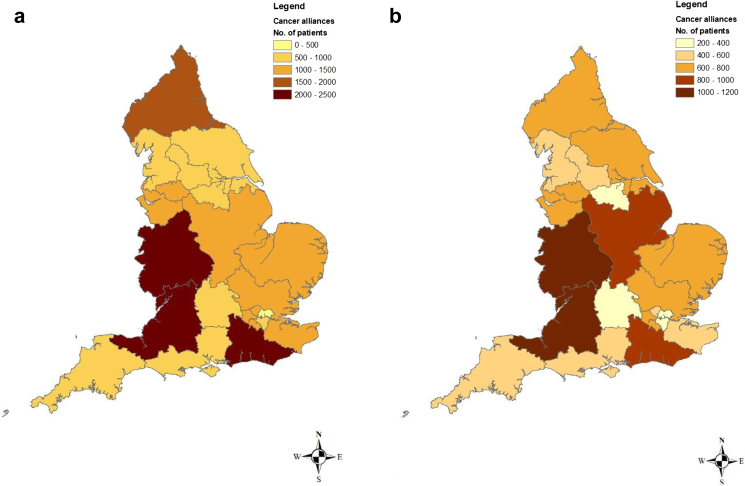
Findings: 100,585 and 49,445 patients underwent breast and colorectal cancer surgery respectively. 67 of 166 hospitals (40.4%) providing breast cancer surgery and 82 of 163 hospitals (50.3%) providing colorectal cancer surgery used less than 80% of their maximum surgical capacity. Hospitals with a 'net loss' of patients to hospitals further away had more potential spare capacity than hospitals with a 'net gain' of patients (p < 0.001 for breast and p = 0.01 for colorectal cancer). At the national level, we projected an annual potential spare capacity of 8389 breast cancer and 4262 colorectal cancer surgical procedures, approximately 25% of the volumes actually performed.
Interpretation: Spare surgical capacity potentially exists in the present configuration of hospitals providing cancer surgery and requires regional allocation for efficient utilisation.
Funding: National Institute for Health Research.
Keywords: Cancer surgery; Capacity; Patient mobility; Treatment backlog; Waiting times.
© 2023 The Authors.
Conflict of interest statement
We declare no competing interests.
Figures
References
-
- Nuffield Trust Cancer waiting times. 2022. https://www.nuffieldtrust.org.uk/resource/cancerwaiting-time-targets Available:
-
- Nossiter J., Morris M., Parry M.G., et al. Impact of the COVID-19 pandemic on the diagnosis and treatment of men with prostate cancer. BJU Int. 2022;130(2):262–270. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
