

Cardiac Tamponade
- PMID: 37465332
- PMCID: PMC10332517
- DOI: 10.21980/J81D1D
Cardiac Tamponade
Abstract
Audience: This simulation is designed to educate emergency medicine residents and medical students on the recognition and management of cardiac tamponade, as well as encourage providers to become familiar with their states' disclosure laws for sentinel events.
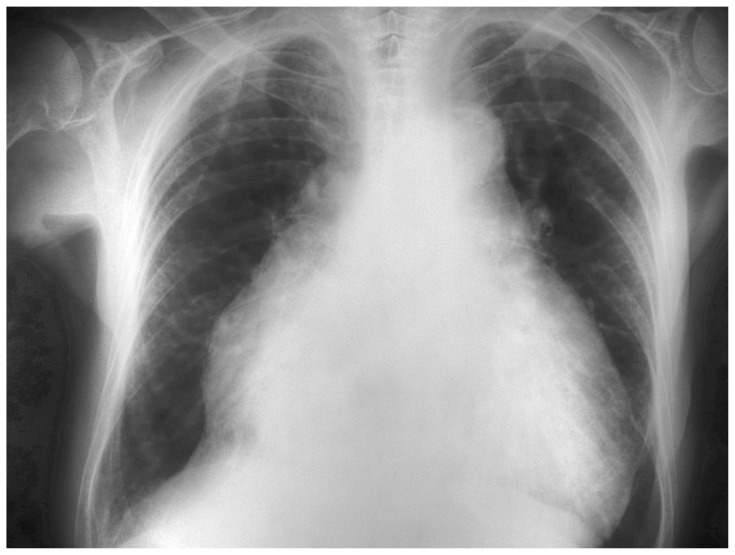
Introduction: Cardiac tamponade is an emergent condition in which the accumulation of pericardial fluid and the consequent increase in hydrostatic pressure becomes severe enough to compromise the normal diastolic and systolic function of the heart, resulting in hemodynamic instability.1 The causes of cardiac tamponade are numerous because it is a potential complication of any of a number of pericardial disease processes, including infectious, inflammatory, traumatic, and malignant etiologies.1,2 Clinical presentations may vary and symptoms can be non-specific, which can lead to delayed or missed diagnoses and poor patient outcomes.3 In addition to this, the incidence of this condition is rising due to the increasing frequency of cardiac procedures performed (ie, pacemaker placement).4 Therefore, it is important for medical providers to have a high index of suspicion for the diagnosis based on patient presentation and to quickly provide necessary treatment to stabilize the patient.
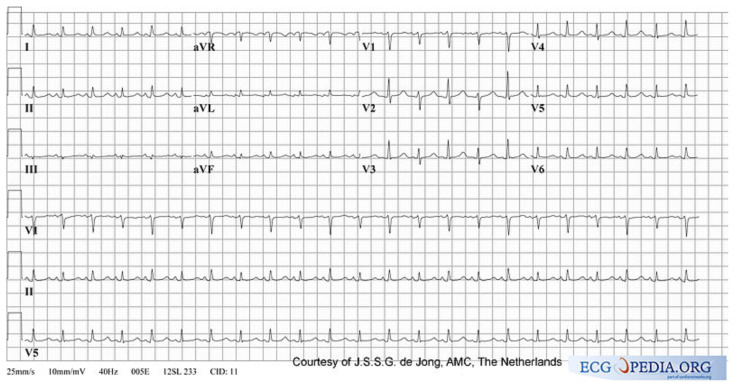
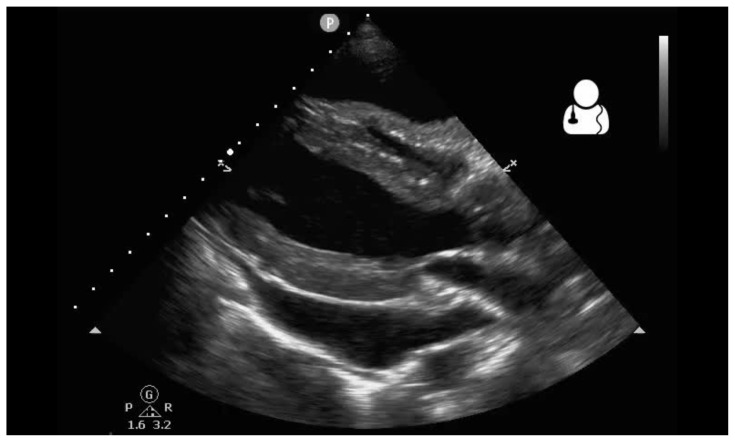
Educational objectives: By the end of this simulation session, the learner will be able to: (1) describe a diagnostic differential for dizziness (2) describe the pathophysiology of cardiac tamponade (3) describe the acute management of cardiac tamponade, including fluid bolus and pericardiocentesis (4) describe the electrocardiogram (ECG) findings of pericardial effusion (5) describe the ultrasound findings of cardiac tamponade (6) describe the indications for emergent bedside pericardiocentesis versus medical stabilization and delayed pericardiocentesis for cardiac tamponade (7) describe the procedural steps for pericardiocentesis, and (8) describe your state's laws regarding disclosure for sentinel events.
Educational methods: This session is conducted using high-fidelity simulation, followed by a debriefing session on evaluation and treatment of cardiac tamponade. However, it may also be run as an oral board case.
Educational methods: Our residents were provided an electronic survey at the completion of the debriefing session so they may rate different aspects of the simulation, as well as provide qualitative feedback on the scenario. This survey is specific to the local institution's simulation center.
Results: Feedback was largely positive because many learners mentioned during debriefing that they are not comfortable with pericardiocentesis and have limited opportunities to practice the procedure. None of our residents were familiar with our state's or institution's disclosure laws for sentinel events.The local institution's simulation center feedback form is based on the Center of Medical Simulation's Debriefing Assessment for Simulation in Healthcare (DASH) Student Version Short Form with the inclusion of required qualitative feedback if an element was scored less than a 6 or 7.5 This session received a majority of 6 (consistently effective/very good) and 7 scores (extremely effective/outstanding).
Discussion: This is a potential method for educating future medical providers on the diagnosis and management of cardiac tamponade in an emergency department setting. Learners initially had a wide range of differentials for the chief complaint of dizziness. We used an ECG with low voltage but without electrical alternans. When asked to provide an ECG interpretation, low voltage was intermittently explicitly interpreted by learners. We were concerned that if we showed an ECG with electrical alternans, learners may quickly arrive at the diagnosis without focusing on the subtleties of a physical exam, including looking for jugular venous distention (JVD) or pulsus paradoxus.We did not have the patient decompensate if their international normalized ratio (INR) was not immediately reversed, given likely delay for in vivo coagulation to occur in the face of life-threatening tamponade, but this provided a robust discussion during debriefing if reversal should be emergently initiated.Many residents voiced that they were uncomfortable performing a pericardiocentesis because they only had a few opportunities to do so on human cadavers, and they appreciated the opportunity to review this.Unexpectedly, when the patient asked the learners if he should sue the cardiologist, the majority of groups told the patient that the cardiologist was not liable because tamponade is a known complication of cardiac ablation and likely reviewed this while obtaining informed consent. None of the learners were familiar with Ohio's disclosure laws for sentinel events. This identified a gap in knowledge that may be addressed in future learning sessions.Our main take-away is to continue providing low-frequency, high-acuity cases that provide the opportunity to review infrequent pathologies and procedures, as well as including patient safety and administrative learning points.
Topics: Medical simulation, cardiac tamponade, pericardial effusion, cardiac emergencies, obstructive shock, sentinel events, iatrogenic injury, medical disclosure.
© 2020 Chu, et al.

Similar articles
-
Spinal Epidural Abscess.J Educ Teach Emerg Med. 2020 Jan 15;5(1):S26-S52. doi: 10.21980/J8T938. eCollection 2020 Jan. J Educ Teach Emerg Med. 2020. PMID: 37465609 Free PMC article.
-
Lightning Strike.J Educ Teach Emerg Med. 2022 Jan 15;7(2):S78-S106. doi: 10.21980/J8SD2M. eCollection 2022 Apr. J Educ Teach Emerg Med. 2022. PMID: 37465437 Free PMC article.
-
Aortic Dissection Presenting as a STEMI.J Educ Teach Emerg Med. 2022 Jul 15;7(3):S26-S54. doi: 10.21980/J8W647. eCollection 2022 Jul. J Educ Teach Emerg Med. 2022. PMID: 37465774 Free PMC article.
-
Pericardial tamponade: A comprehensive emergency medicine and echocardiography review.Am J Emerg Med. 2022 Aug;58:159-174. doi: 10.1016/j.ajem.2022.05.001. Epub 2022 May 6. Am J Emerg Med. 2022. PMID: 35696801 Review.
-
Does this patient with a pericardial effusion have cardiac tamponade?JAMA. 2007 Apr 25;297(16):1810-8. doi: 10.1001/jama.297.16.1810. JAMA. 2007. PMID: 17456823 Review.
References
-
- Debriefing Assessment for Simulation in Healthcare (DASH) Center for Medical Simulation; [Accessed April 25, 2020]. https://harvardmedsim.org/debriefing-assessment-for-simulation-in-health...
LinkOut - more resources
Full Text Sources
Miscellaneous