

Necrotizing Fasciitis
- PMID: 37465410
- PMCID: PMC10332573
- DOI: 10.21980/J84M1D
Necrotizing Fasciitis
Abstract
Audience: This scenario was developed to educate emergency medicine residents and medical students on the diagnosis and management of necrotizing fasciitis (NF).
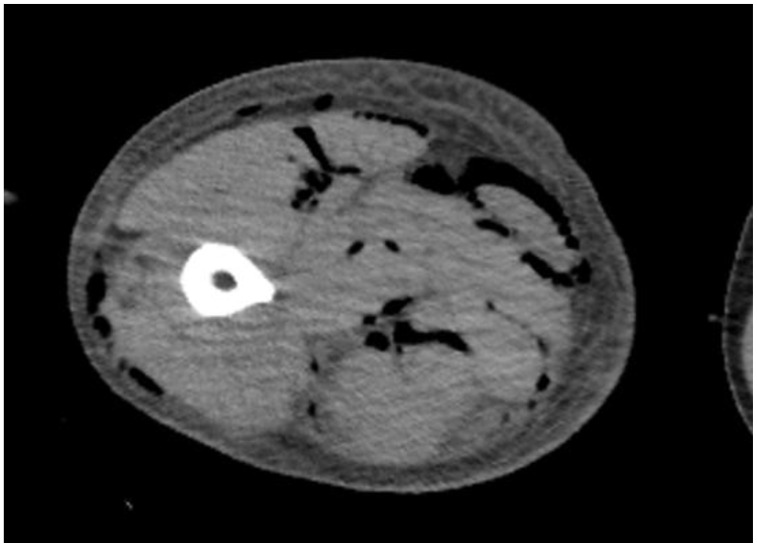
Introduction: Necrotizing fasciitis is an uncommon and life-threatening deep tissue infection. Clinical presentations may range from subtle non-specific signs and symptoms to multi-organ failure.1 Signs and symptoms suggestive of necrotizing fasciitis include skin necrosis, hemorrhagic bullae, pain out of proportion, and erythema progressing beyond margins.2 Radiographs may show dissecting gas along fascial planes in the absence of trauma, but this is not a sensitive finding and may present late in the disease course. Ultrasound may demonstrate soft-tissue gas, fascial irregularity, and diffuse fascial thickening. Computerized tomography (CT) is the imaging modality of choice. The sensitivity of diagnosing necrotizing infections on CT is 80% and the diagnosis should not be excluded by lack of soft tissue gas.3 While laboratory findings may reveal an elevated C-reactive protein (CRP) level,4 other laboratory findings may be used in conjunction to calculate a laboratory risk indicator for necrotizing soft tissue infections score (LRINEC) value which may predict morbidity and mortality.5 Providers must treat empirically without delay or confirmation through laboratory results or imaging studies. Treatment should be initiated in a timely fashion, including broad-spectrum antibiotics, intravenous fluids, and urgent discussion with surgical consultants to evaluate for prompt operative management.6.
Educational objectives: At the conclusion of the simulation session, learners will be able to: 1) Describe the spectrum of clinical presentations of necrotizing fasciitis. 2) Identify the microbial etiology of necrotizing fasciitis. 3) Describe the empiric antibiotics appropriate for necrotizing fasciitis. 4) Describe benefits and limitations of various imaging studies when working up necrotizing fasciitis.
Educational methods: This session was conducted using high-fidelity simulation, followed by a debriefing session reviewing case progression, differential diagnoses, management, and disposition. This scenario may also be run as an oral boards case.
Research methods: Our residents are provided a survey at the completion of the debriefing session so they may rate different aspects of the simulation, as well as provide qualitative feedback on the scenario.
Results: Residents were also asked to rate the overall clinical experience of the simulation activity on a scale of 1 to 7; 1 being extremely ineffective/detrimental and 7 being extremely effective/outstanding. A total of 10 resident participants responded to the survey. This simulation scenario had a median rating of 7 for the instructor setting the stage and for instructors introducing themselves and explaining the learning objectives. A median rating of 7 was also given in explaining the strength and weakness of the simulation scenario, which was key to its clinical application.Residents voiced appreciation that the clinical presentation was unique and that it required a thorough physical exam, including visualizing the affected area. As the patient presented rather early in his clinical course, they felt the diagnosis was more difficult to ascertain, as rhabdomyolysis and cellulitis were also on their differentials.
Discussion: This is a cost-effective method to review a presentation of necrotizing fasciitis early in the disease course. Since the patient did not have a high fever or toxic appearance, participants demonstrated some hesitation in definitively diagnosing a necrotizing infection. We will continue to provide simulation scenarios with more subtle or early presentations to challenge residents' diagnostic skills.
Topics: Medical simulation, soft tissue infection, necrotizing fasciitis, infectious disease.
© 2020 Desta, et al.


Similar articles
-
Spinal Epidural Abscess.J Educ Teach Emerg Med. 2020 Jan 15;5(1):S26-S52. doi: 10.21980/J8T938. eCollection 2020 Jan. J Educ Teach Emerg Med. 2020. PMID: 37465609 Free PMC article.
-
Cervical Necrotizing Fasciitis, Diagnosis and Treatment of a Rare Life-Threatening Infection.Ear Nose Throat J. 2023 Mar;102(3):NP109-NP113. doi: 10.1177/0145561321991341. Epub 2021 Feb 11. Ear Nose Throat J. 2023. PMID: 33570428
-
Cardiac Tamponade.J Educ Teach Emerg Med. 2020 Oct 15;5(4):S84-S107. doi: 10.21980/J81D1D. eCollection 2020 Oct. J Educ Teach Emerg Med. 2020. PMID: 37465332 Free PMC article.
-
Necrotizing Soft Tissue Infections (NSTI): Pearls and Pitfalls for the Emergency Clinician.J Emerg Med. 2022 Apr;62(4):480-491. doi: 10.1016/j.jemermed.2021.12.012. Epub 2022 Jan 31. J Emerg Med. 2022. PMID: 35115188 Review.
-
Using clinical pathways to aid in the diagnosis of necrotizing soft tissue infections synthesis of evidence.Worldviews Evid Based Nurs. 2012 Apr;9(2):88-99. doi: 10.1111/j.1741-6787.2011.00235.x. Epub 2011 Dec 12. Worldviews Evid Based Nurs. 2012. PMID: 22151905 Review.
Cited by
-
Distribution of Necrotizing fasciitis Using the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) Score Among Patients Attending a Tertiary Hospital in Chennai.Cureus. 2024 Nov 15;16(11):e73755. doi: 10.7759/cureus.73755. eCollection 2024 Nov. Cureus. 2024. PMID: 39677092 Free PMC article.
-
Periorbital Necrotizing Fasciitis: Presentation to Reconstruction.Cureus. 2024 May 2;16(5):e59501. doi: 10.7759/cureus.59501. eCollection 2024 May. Cureus. 2024. PMID: 38826916 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous