

Pulseless Electrical Activity Cardiac Arrest
- PMID: 37465603
- PMCID: PMC10332535
- DOI: 10.21980/J8Z055
Pulseless Electrical Activity Cardiac Arrest
Abstract
Audience: This simulation-based scenario is appropriate for senior level emergency medicine residents.
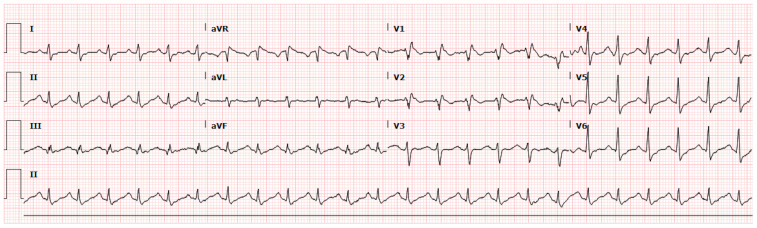
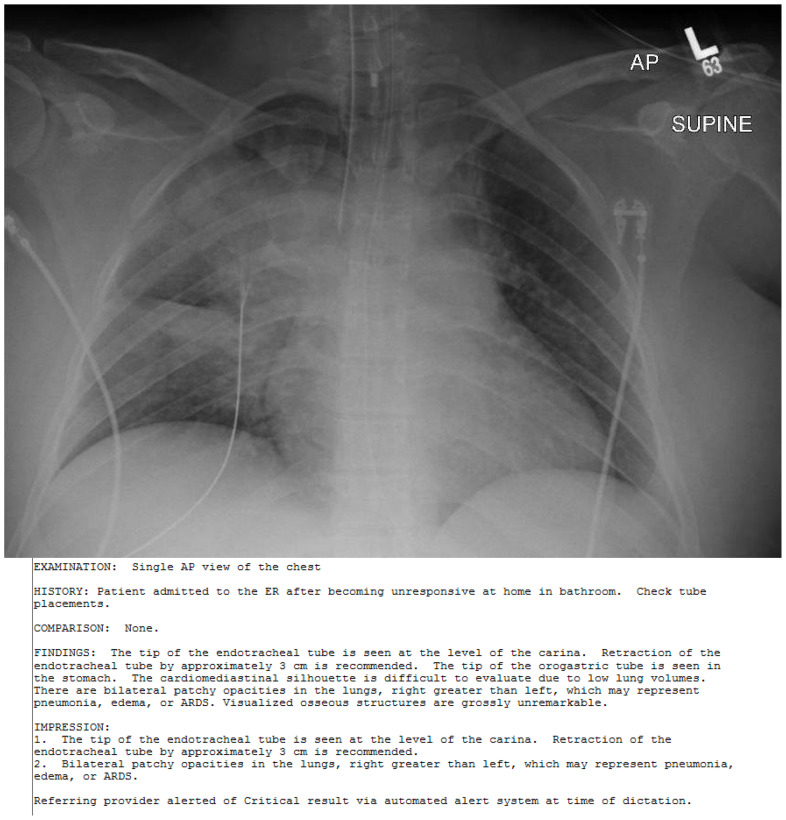
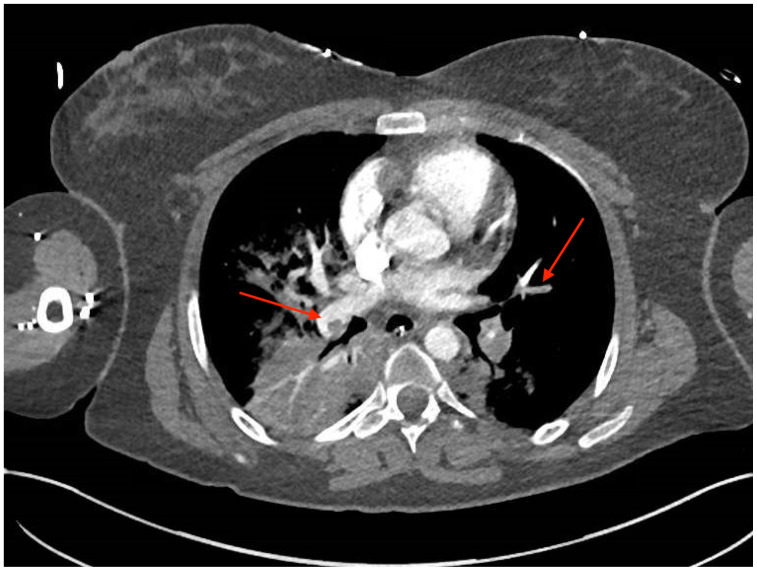
Introduction: Pulseless electrical activity (PEA) accounts for up to 25% of sudden cardiac arrest;1 therefore the ability to recognize and care for this condition is an essential skill of emergency medicine physicians. Management of PEA arrest in the emergency department centers on Advanced Cardiac Life Support (ACLS) algorithms and the identification and treatment of potentially reversible causes. Massive pulmonary embolism (PE) is one of several causes of PEA cardiac arrest.2 However, diagnosis by CT-angiographic or nuclear imaging may not be obtainable in the hemodynamically unstable patient, requiring physicians to have a high index of suspicion. Systemic thrombolytic therapy is indicated in cardiac arrest due to known or presumed massive pulmonary embolism.3,4,5.
Educational objectives: After competing this simulation-based session, the learner will be able to:Identify PEA arrestReview the ACLS commonly recognized PEA arrest etiologies via the H &T mnemonicReview and discuss the risks and benefits of tissue plasminogen activator (tPA) for massive PE.
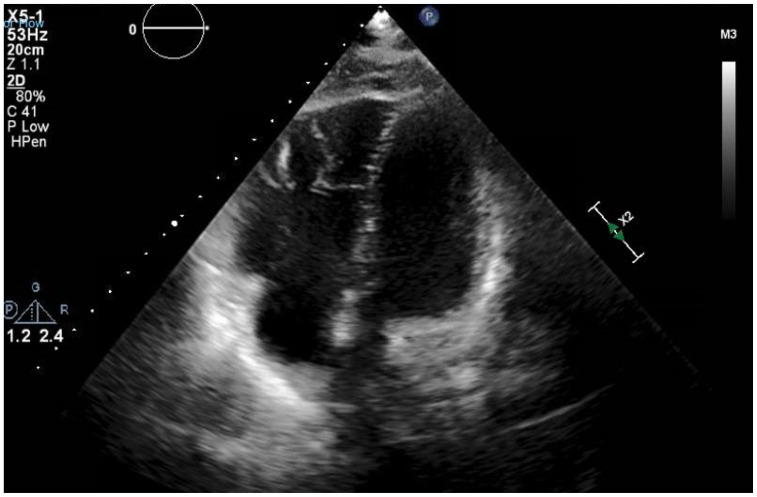
Educational methods: This is a high-fidelity simulation that allows learners to evaluate and treat a PEA arrest secondary to massive PE in a safe environment. The learners will demonstrate their ability to recognize a PEA arrest, sort through possible etiologies, and demonstrate treatment of a massive PE with tPA. Debriefing will focus on diagnosis and management of the PEA arrest.
Research methods: This case was piloted with 12 PGY-2 and PGY-3 residents. Group and individual debriefing occurred post-case.
Results: Post-simulation feedback from the faculty suggested two potential issues. First was fidelity, which we increased by using our ultrasound simulator. Second, the elevated presenting glucose with lactic acidosis could be a poor cue, leading some towards diabetic ketoacidosis (DKA).
Discussion: Learners felt more confident about running a PEA arrest. The simulation improved resident awareness of the value of point of care ultrasound (POCUS) in cardiac arrest. It also clarified the dosing of tPA in massive PE. Faculty felt simulating the actual US without breaking simulation would be more challenging without our US simulator. Although there was concern about results pointing towards possible DKA, this did not occur in any of the pilot simulations. The presenting glucose was reduced to make this less likely in future simulations.
Topics: Pulseless electrical activity (PEA), syncope, cardiac arrest, Hs and Ts from ACLS PEA instruction, tPA for massive PE, critical care medicine, simulation.
© 2020 Sembroski, et al.
Similar articles
-
Hemoptysis Due to Diffuse Alveolar Hemorrhage.J Educ Teach Emerg Med. 2020 Jul 15;5(3):S1-S27. doi: 10.21980/J8ZP86. eCollection 2020 Jul. J Educ Teach Emerg Med. 2020. PMID: 37465227 Free PMC article.
-
Extracorporeal Membrane Oxygenation (ECMO) for Refractory Cardiac Arrest.J Educ Teach Emerg Med. 2020 Oct 15;5(4):S28-S58. doi: 10.21980/J88W69. eCollection 2020 Oct. J Educ Teach Emerg Med. 2020. PMID: 37465336 Free PMC article.
-
Cardiac Arrest in an Adolescent with Pulmonary Embolism.J Educ Teach Emerg Med. 2021 Oct 15;6(4):S112-S137. doi: 10.21980/J8135T. eCollection 2021 Oct. J Educ Teach Emerg Med. 2021. PMID: 37465265 Free PMC article.
-
Unveiling pseudo-pulseless electrical activity (pseudo-PEA) in ultrasound-integrated infant resuscitation.Eur J Pediatr. 2023 Dec;182(12):5285-5291. doi: 10.1007/s00431-023-05199-3. Epub 2023 Sep 19. Eur J Pediatr. 2023. PMID: 37725211 Free PMC article. Review.
-
Pseudo-pulseless electrical activity in the emergency department, an evidence based approach.Am J Emerg Med. 2020 Feb;38(2):371-375. doi: 10.1016/j.ajem.2019.158503. Epub 2019 Oct 14. Am J Emerg Med. 2020. PMID: 31740090 Review.
Cited by
-
Point-of-Care Ultrasonography Detects Vanishing Air Embolism Following Central Venous Catheter Removal in a Patient With Chest Tube Drainage: A Case Report.Clin Case Rep. 2025 Jun 30;13(7):e70578. doi: 10.1002/ccr3.70578. eCollection 2025 Jul. Clin Case Rep. 2025. PMID: 40589666 Free PMC article.
References
References/suggestions for further reading
-
- Podrid PJ. Pathophysiology and etiology of sudden cardiac arrest. In: Olshansky B, Manaker S, Downey BC, editors. UpToDate. Waltham, MA: UpToDate Inc; https://www.uptodate.com/contents/pathophysiologyand-etiology-of-sudden-.... Updated Apr 18, 2018.
-
- Kline JA. Venous Thromboembolism. In: Tintinalli JE, Stapczynski JS, Ma OJ, et al., editors. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 8th ed. New York, NY: McGraw-Hill; 2016. pp. 388–398.
-
- Kasper W, Konstantinides S, Geibel A, et al. Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. J Am Coll Cardiol. 1997;30(5):1165–1171. - PubMed
Further reading
-
- DePalo VA, Kharnaf AE.Panchbhavi VK, editor. Venous Thromboembolism (VTE) Treatment & Management. Medscape. [Accessed July 2, 2019]. https://emedicine.medscape.com/article/1267714-treatment#d10. Published June 12, 2019.
-
- Kline JA. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 9th ed. Philadelphia, PA: Elsevier Inc; 2018. [Accessed October 30, 2019]. Pulmonary Embolism and Deep Vein Thrombosis. https://www-clinicalkeycom.siumed.idm.oclc.org/#!/content/book/3-s2.0-B9... .
-
- Nickson C.Thrombolysis for submassive pulmonary embolus. Life in the FastLane. [Accessed July 2, 2019]. https://litfl.com/thrombolysis-for-submassive-pulmonary-embolus/. Published June 9, 2019.
-
- Shah SN, Kharnaf AE.Dizon JM, editor. Pulseless Electrical Activity. Medscape. [Accessed October 30, 2019]. https://emedicine.medscape.com/article/161080-overview. Published March 27, 2018.
-
- Tapson VF, Weinberg AS. Thrombolytic (fibrinolytic) therapy in acute pulmonary embolism and lower extremity deep vein thrombosis. In: Mandel J, Finlay G, editors. UpToDate. Waltham, MA: 2019. https://www.uptodate.com/contents/search?search=thrombolytic-fibrinolyti.... Updated May 3, 2019.