

Virtual 3D Specimen Mapping in Head & Neck Oncologic Surgery
- PMID: 37466329
- PMCID: PMC10796840
- DOI: 10.1002/lary.30881
Virtual 3D Specimen Mapping in Head & Neck Oncologic Surgery
Abstract
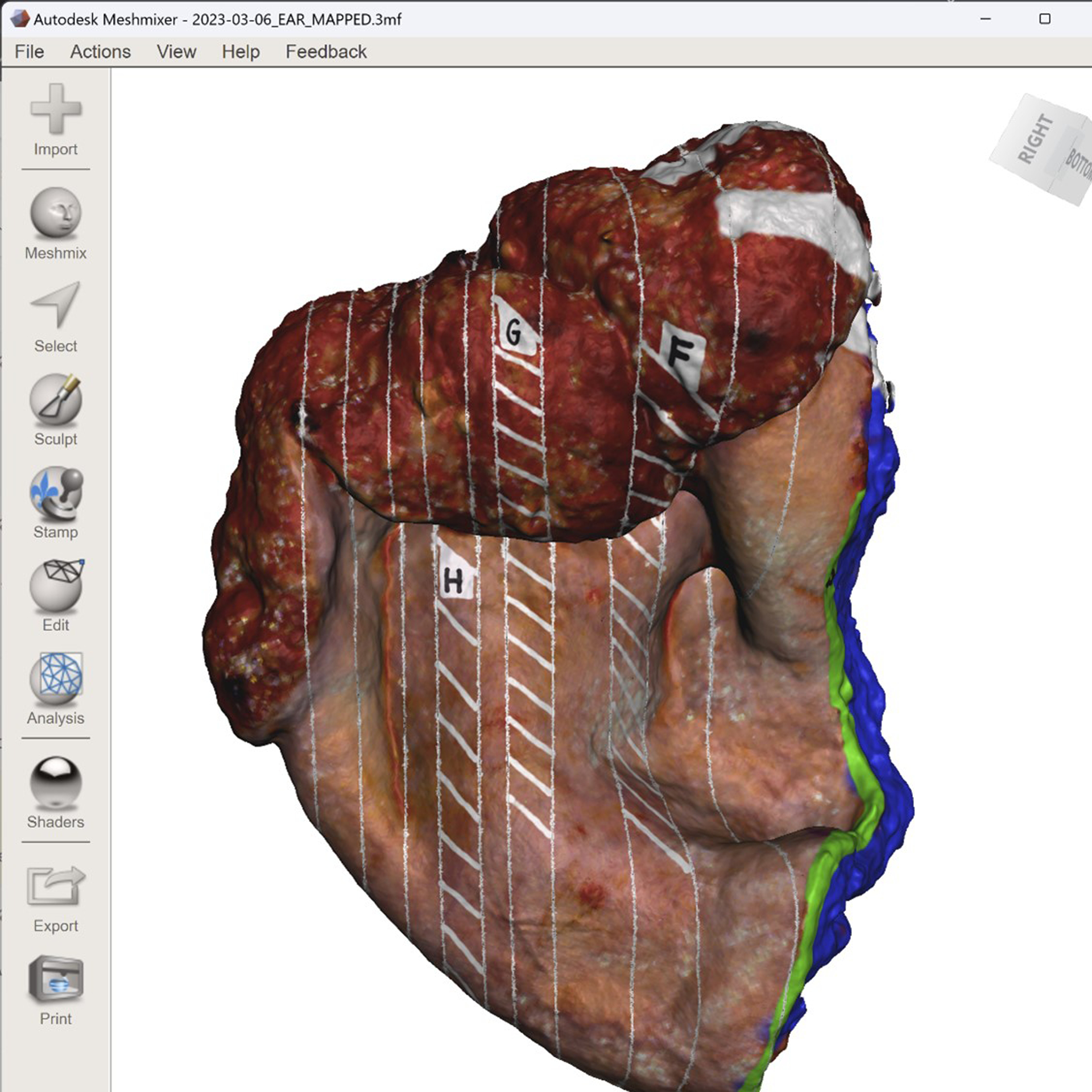
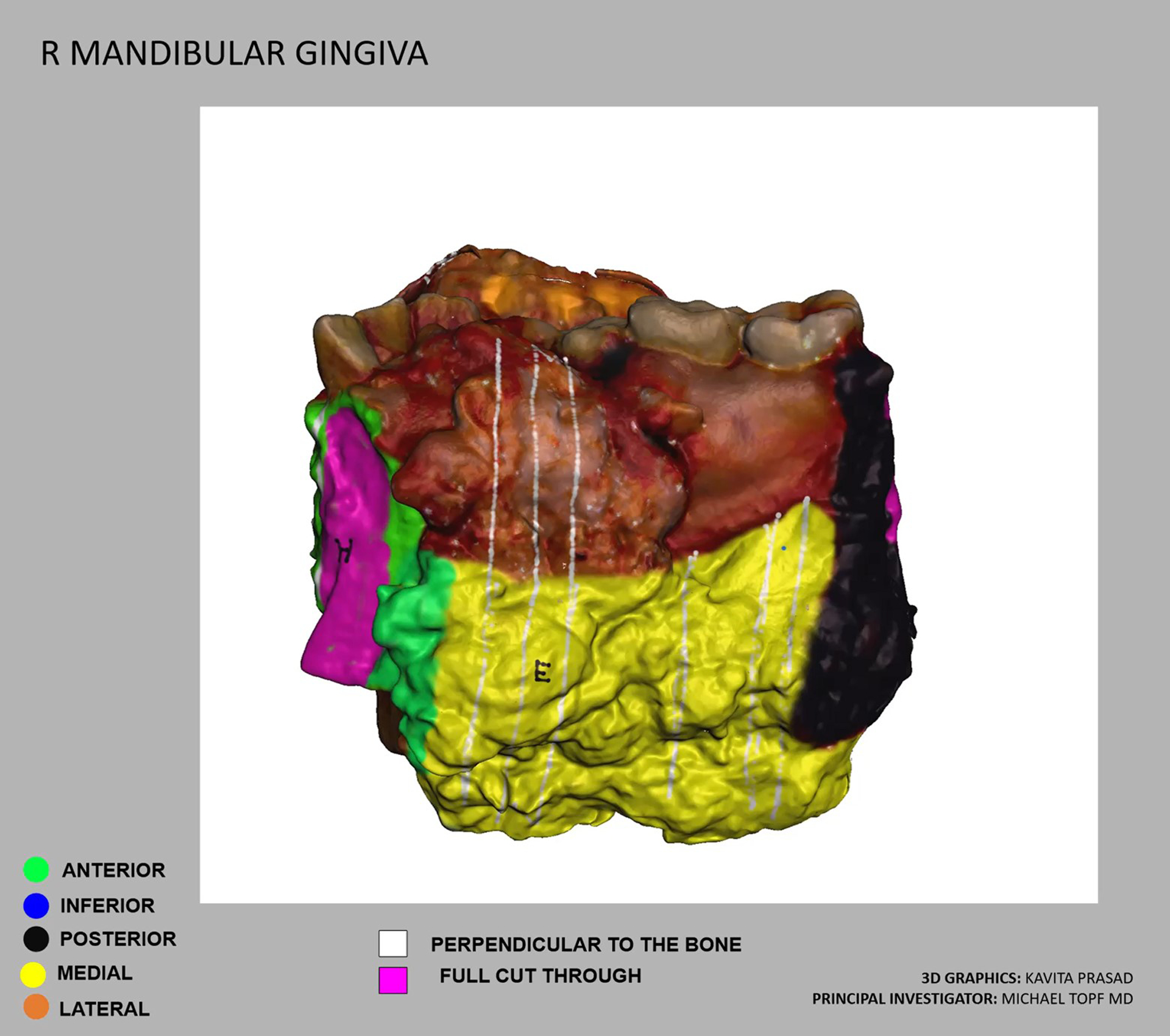
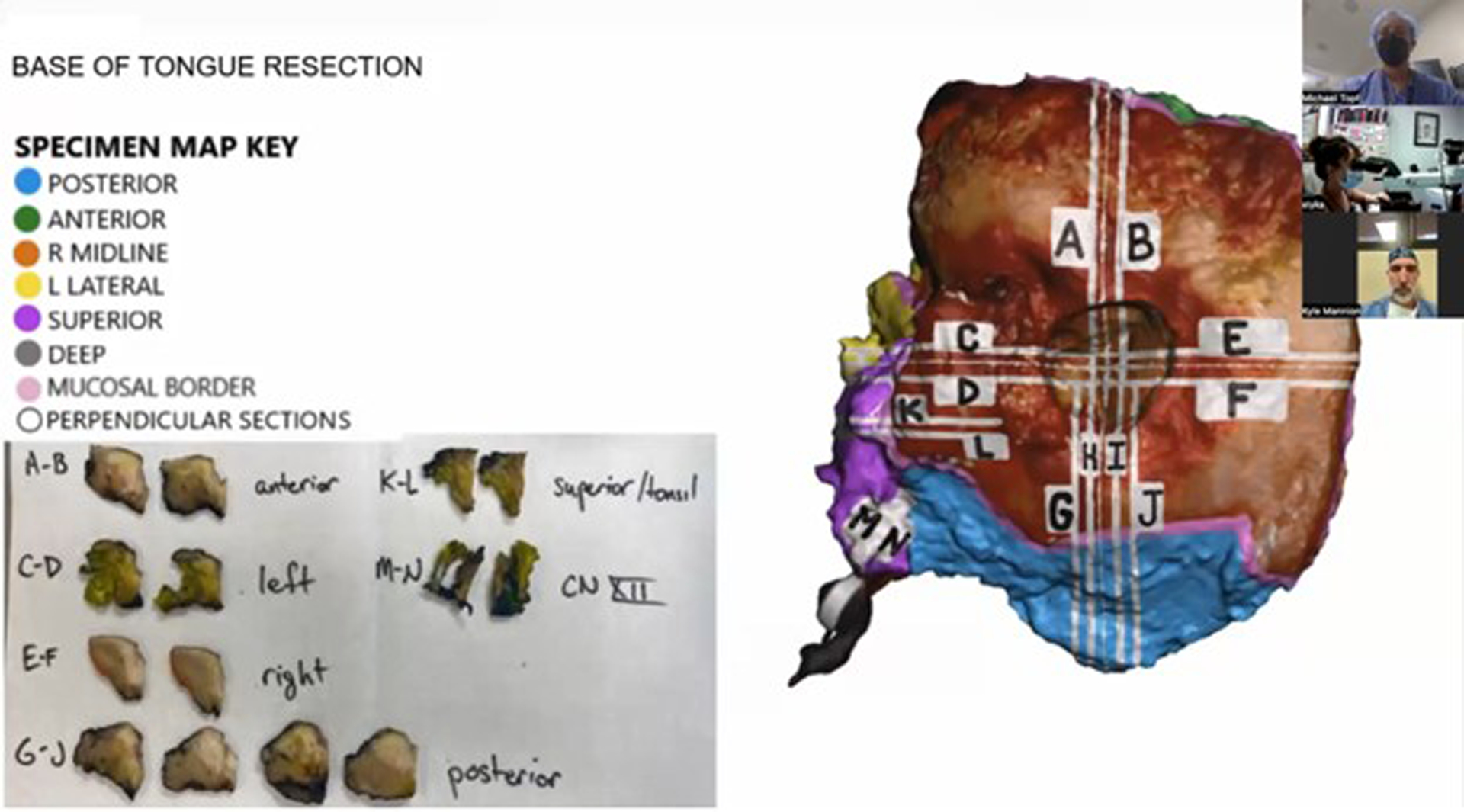
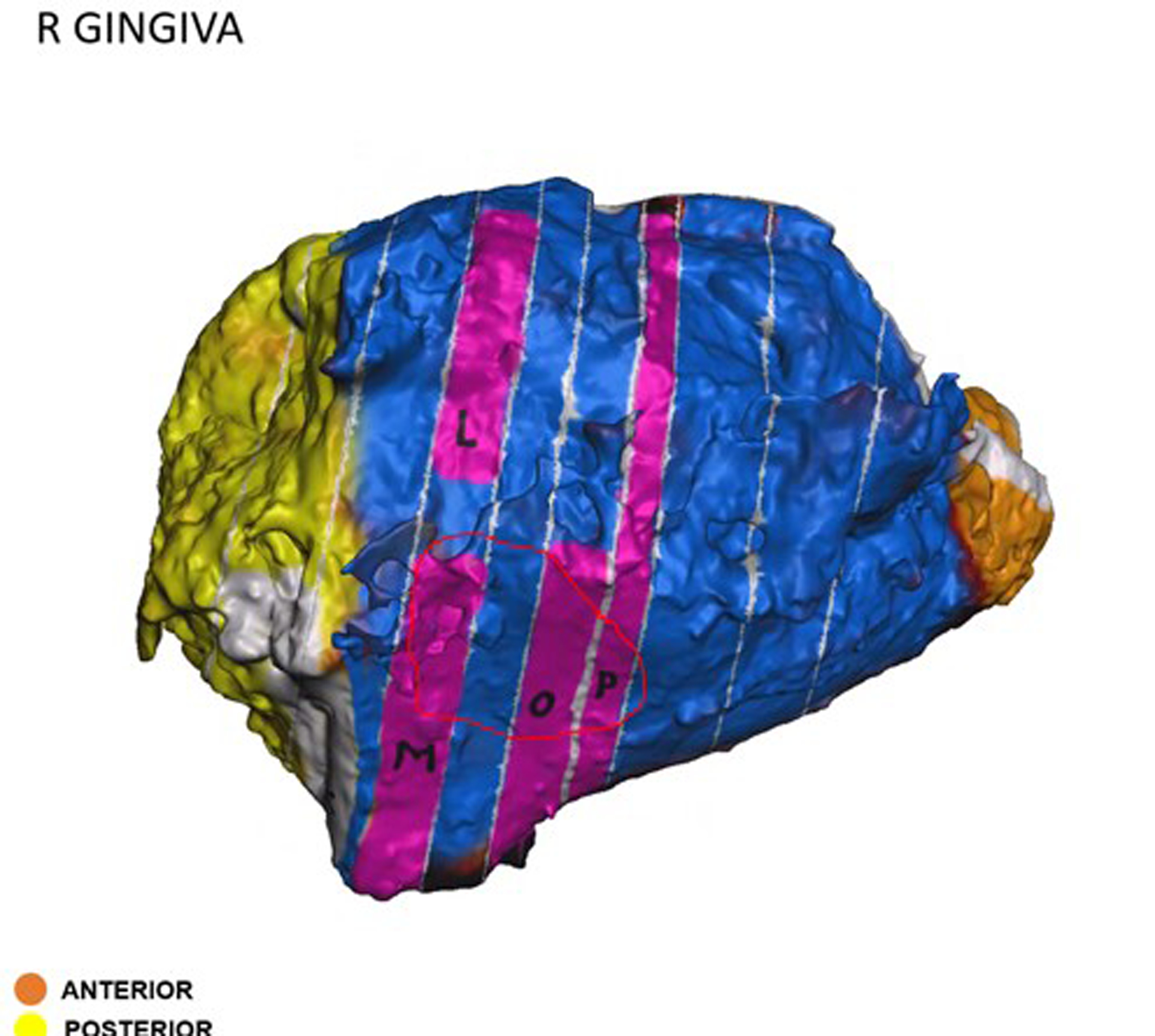
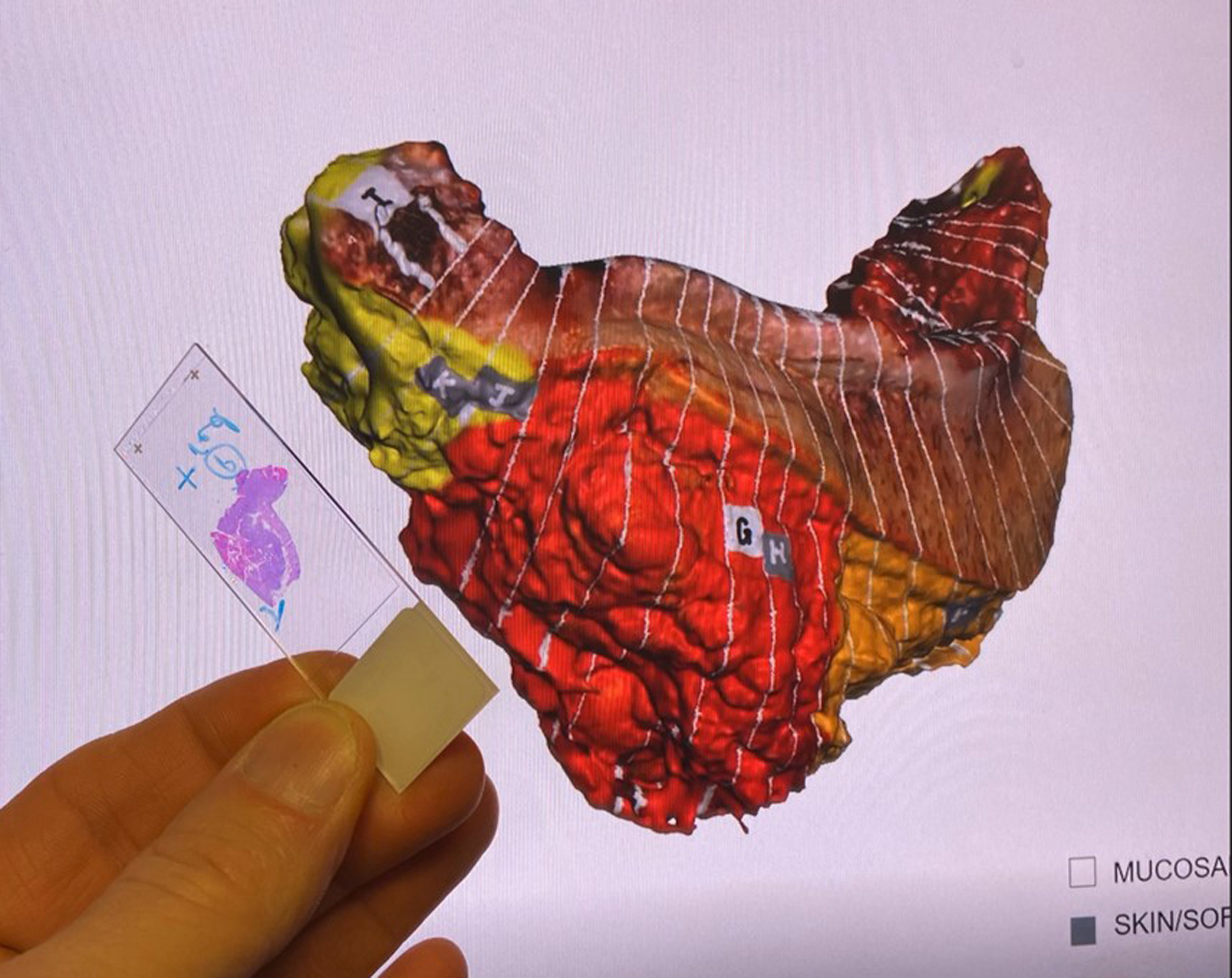
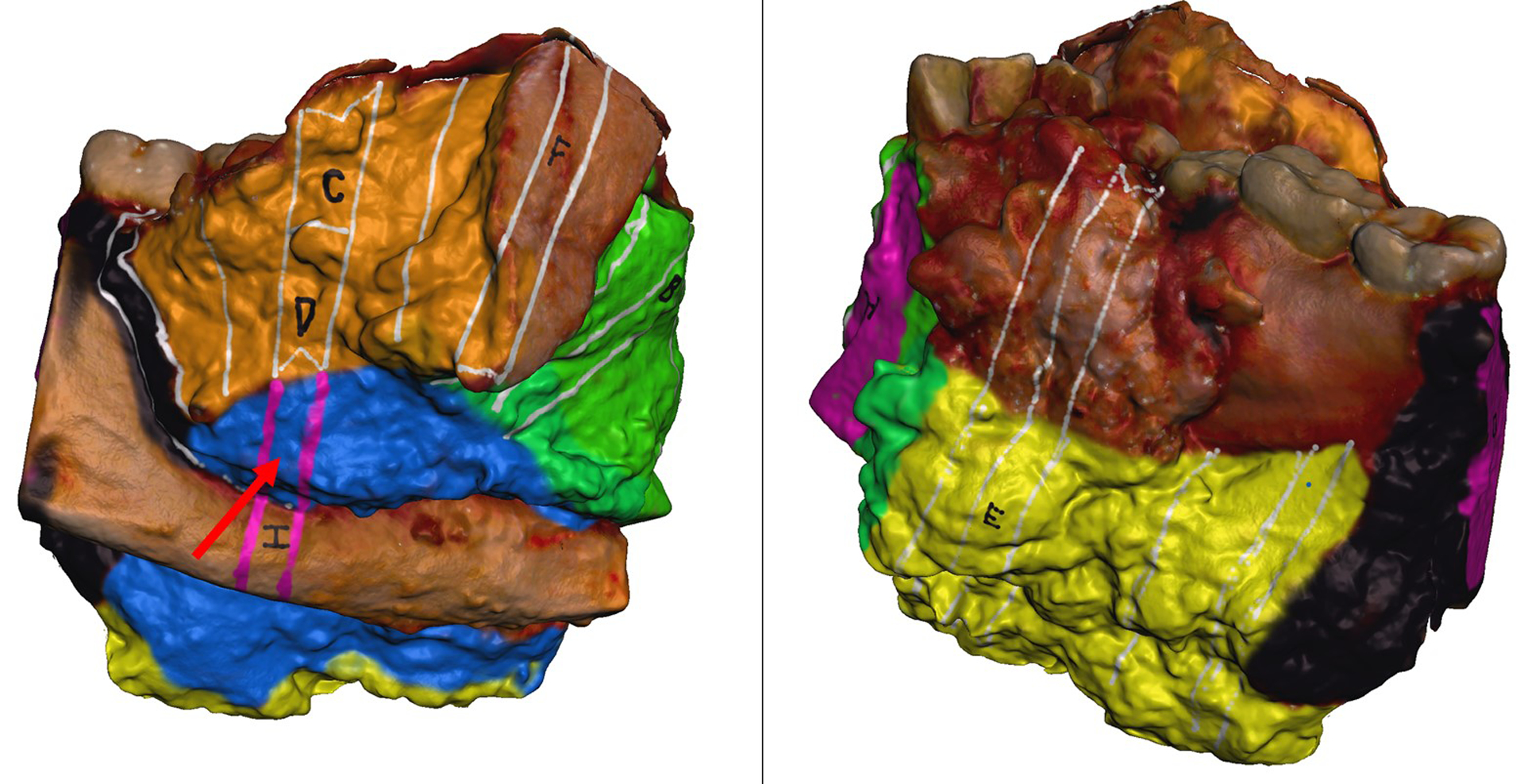
Objectives: Virtual 3D specimen mapping of oncologic surgical specimens provides a visual record of the specimen and margin sampling sites which can be utilized in a variety of cancer care settings. Our objective was to perform a retrospective review of head and neck surgical oncology cases where the specimen was mapped post-operatively and to evaluate the utility of these 3D specimen maps amongst the multidisciplinary cancer care team.
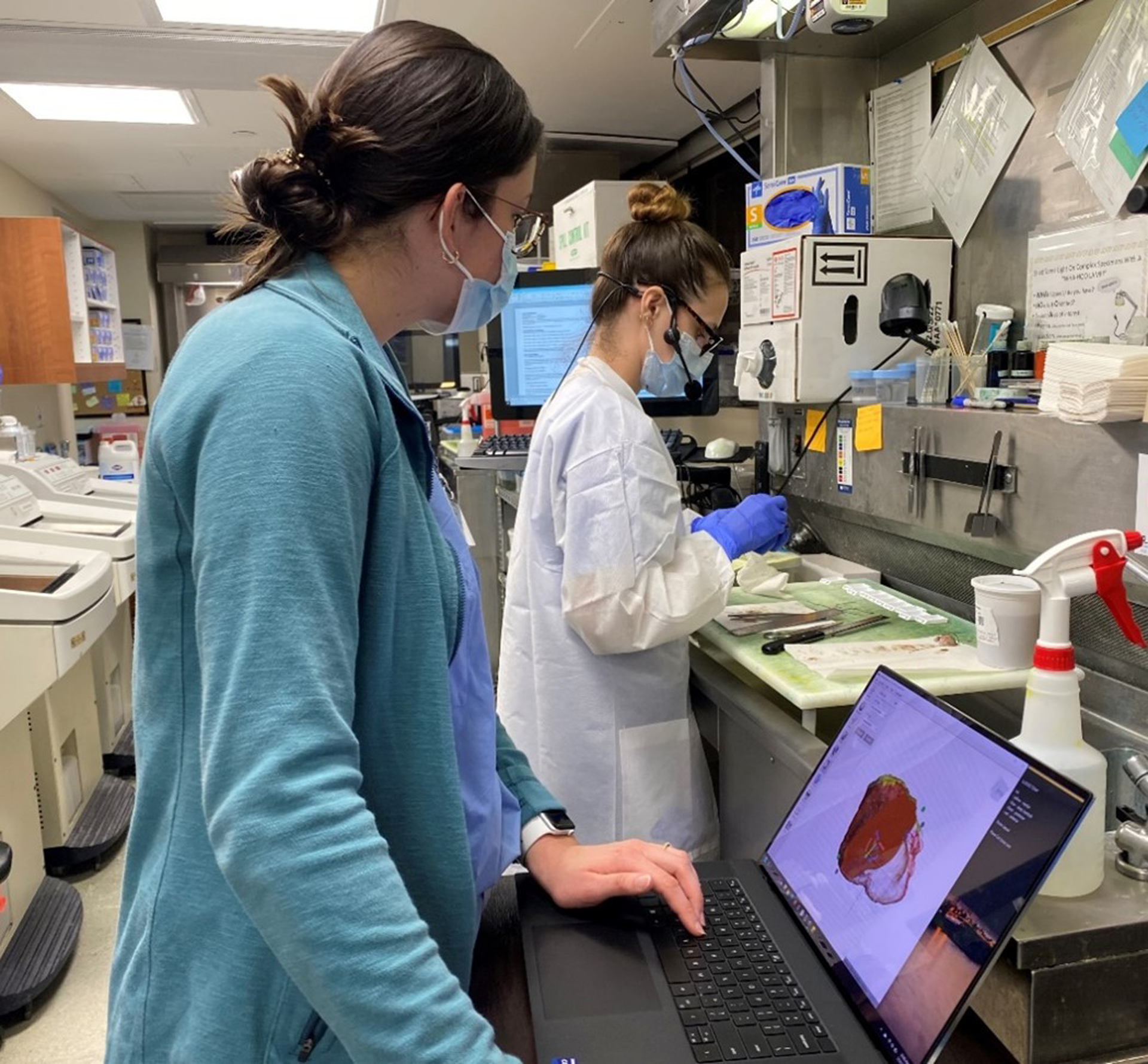
Methods: A retrospective review of our 3D specimen model biorepository was performed. Surgical specimens were 3D scanned and then graphically annotated (or "mapped") during routine pathologic processing. The resulting 3D specimen maps were distributed to the multidisciplinary oncologic care team. Final margin status and any use of the 3D specimen maps were recorded.
Results: A total of 28 cases were included. Virtual 3D specimen maps were utilized by the cancer care team in 8 cases (29%), including 2 positive margin cases, 2 close margin cases, and 4 indeterminate margin cases. 3D specimen maps were used to visualize positive margin sites for pathologist-surgeon communication as a visual reference during tumor board discussions and to inform radiation treatment planning.
Conclusion: Post-operative virtual 3D specimen mapping of oncologic specimens creates a permanent visual record of the specimen and the margins sampled and may serve as a beneficial tool for communication amongst the multidisciplinary cancer care team.
Level of evidence: 4 Laryngoscope, 134:191-197, 2024.
Keywords: 3D scanning; head and neck cancer; pathology communication; surgical margins.
© 2023 The American Laryngological, Rhinological and Otological Society, Inc.
Conflict of interest statement
Figures
Similar articles
-
Digital mapping of resected cancer specimens: The visual pathology report.J Pathol Inform. 2024 Sep 28;15:100399. doi: 10.1016/j.jpi.2024.100399. eCollection 2024 Dec. J Pathol Inform. 2024. PMID: 39712976 Free PMC article.
-
Visual pathology reports for communication of final margin status in laryngeal cancer surgery.J Pathol Inform. 2024 Oct 28;15:100404. doi: 10.1016/j.jpi.2024.100404. eCollection 2024 Dec. J Pathol Inform. 2024. PMID: 39640916 Free PMC article.
-
Enhanced Communication of Tumor Margins Using 3D Scanning and Mapping.J Vis Exp. 2023 Dec 15;(202). doi: 10.3791/66253. J Vis Exp. 2023. PMID: 38163271
-
Intraoperative Margin Assessment in Head and Neck Cancer: A Case of Misuse and Abuse?Head Neck Pathol. 2020 Jun;14(2):291-302. doi: 10.1007/s12105-019-01121-2. Epub 2020 Mar 2. Head Neck Pathol. 2020. PMID: 32124417 Free PMC article. Review.
-
Retroperitoneal margin of the pancreaticoduodenectomy specimen: anatomic mapping for the surgical pathologist.Virchows Arch. 2009 Feb;454(2):125-31. doi: 10.1007/s00428-008-0711-9. Epub 2008 Dec 6. Virchows Arch. 2009. PMID: 19066952 Review.
Cited by
-
Digital mapping of resected cancer specimens: The visual pathology report.J Pathol Inform. 2024 Sep 28;15:100399. doi: 10.1016/j.jpi.2024.100399. eCollection 2024 Dec. J Pathol Inform. 2024. PMID: 39712976 Free PMC article.
-
Visual pathology reports for improved collaboration at multidisciplinary head and neck tumor board.Head Neck. 2025 Feb;47(2):452-462. doi: 10.1002/hed.27926. Epub 2024 Aug 29. Head Neck. 2025. PMID: 39206523 Free PMC article.
-
3D Scanning of Surgical Specimens to Improve Communication Between Surgeon and Pathologist: A Head and Neck Pilot Study.Cancers (Basel). 2024 Dec 24;17(1):14. doi: 10.3390/cancers17010014. Cancers (Basel). 2024. PMID: 39796645 Free PMC article.
-
Augmented Reality-Guided Frozen Section Analysis: Bringing the Pathologist From the Laboratory to the Operating Room.OTO Open. 2024 Aug 28;8(3):e70002. doi: 10.1002/oto2.70002. eCollection 2024 Jul-Sep. OTO Open. 2024. PMID: 39206428 Free PMC article.
-
Visual pathology reports for communication of final margin status in laryngeal cancer surgery.J Pathol Inform. 2024 Oct 28;15:100404. doi: 10.1016/j.jpi.2024.100404. eCollection 2024 Dec. J Pathol Inform. 2024. PMID: 39640916 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
