

Long-term survival following transvenous lead extraction: unpicking differences according to sex
- PMID: 37466333
- PMCID: PMC10410196
- DOI: 10.1093/europace/euad214
Long-term survival following transvenous lead extraction: unpicking differences according to sex
Abstract
Aims: Female sex is a recognized risk factor for procedure-related major complications including in-hospital mortality following transvenous lead extraction (TLE). Long-term outcomes following TLE stratified by sex are unclear. The purpose of this study was to evaluate factors influencing long-term survival in patients undergoing TLE according to sex.
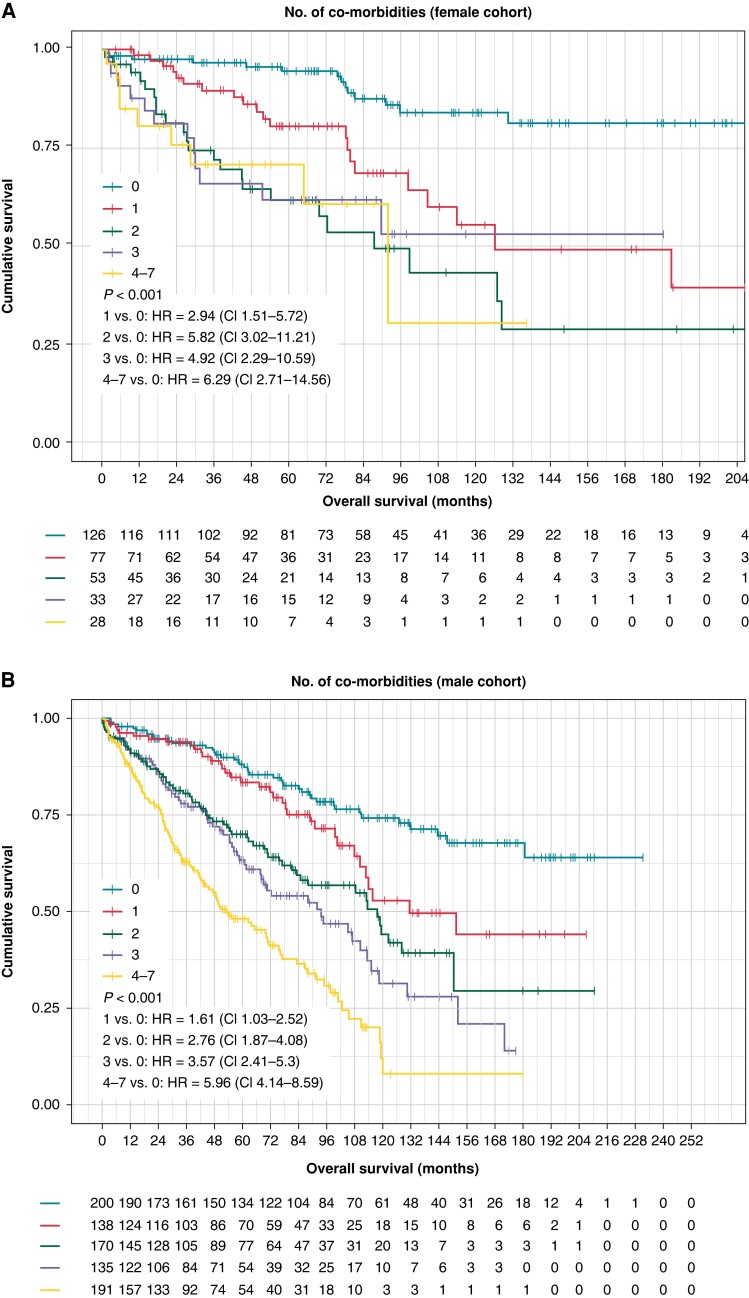
Methods and results: Clinical data from consecutive patients undergoing TLE in the reference centre between 2000 and 2019 were prospectively collected. The total cohort was divided into groups based on sex. We evaluated the association of demographic, clinical, device-related, and procedure-related factors on long-term mortality. A total of 1151 patients were included, with mean 66-month follow-up and mortality of 34.2% (n = 392). The majority of patients were male (n = 834, 72.4%) and 312 (37.4%) died. Males were more likely to die on follow-up [hazard ratio (HR) = 1.58 (1.23-2.02), P < 0.001]. Males had a higher mean age at explant (66.2 ± 13.9 vs. 61.3 ± 16.3 years, P < 0.001), greater mean co-morbidity burden (2.14 vs. 1.27, P < 0.001), and lower mean left ventricular ejection fraction (LVEF) (43.4 ± 14.0 vs. 50.8 ± 12.7, P = 0.001). For the female cohort, age > 75 years [HR = 3.45 (1.99-5.96), P < 0.001], estimated glomerular filtration rate < 60 [HR = 1.80 (1.03-3.11), P = 0.037], increasing co-morbidities (HR = 1.29 (1.06-1.56), P = 0.011), and LVEF per percentage increase [HR = 0.97 (0.95-0.99), P = 0.005] were all significant factors predicting mortality. The same factors influenced mortality in the male cohort; however, the HRs were lower.
Conclusion: Female patients undergoing TLE have more favourable long-term outcomes than males with lower long-term mortality. Similar factors influenced mortality in both groups.
Keywords: Infection; Mortality; Prognosis; Sex; TLE; Transvenous lead extraction.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: N.W. receives fellowship funding from the British Heart Foundation (FS/CRTF/22/24362). V.S.M. has received fellowship funding from Siemens and Abbott. S.A.N. acknowledges support from the UK Engineering and Physical Sciences Research Council (EP/M012492/1, NS/A000049/1, and EP/P01268X/1), the British Heart Foundation (PG/15/91/31812, PG/13/37/30280, and SP/18/6/33805), US National Institutes of Health (NIH R01-HL152256), European Research Council (ERC PREDICT-HF 864055), and Kings Health Partners London National Institute for Health Research (NIHR) Biomedical Research Centre. C.A.R. receives research funding and/or consultation fees from Abbott, Medtronic, Boston Scientific, Spectranetics, and MicroPort outside of the submitted work.
Figures




References
-
- Raatikainen MJP, Arnar DO, Merkely B, Nielsen JC, Hindricks G, Heidbuchel Het al. . A decade of information on the use of cardiac implantable electronic devices and interventional electrophysiological procedures in the European Society of Cardiology countries: 2017 report from the European Heart Rhythm Association. Europace 2017;19:ii1–ii90. - PubMed
-
- Kusumoto FM, Schoenfeld MH, Wilkoff BL, Berul CI, Birgersdotter-Green UM, Carrillo Ret al. . 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm 2017;14:e503–51. - PubMed
-
- Bongiorni MG, Kennergren C, Butter C, Deharo JC, Kutarski A, Rinaldi CAet al. . The European Lead Extraction ConTRolled (ELECTRa) study: a European Heart Rhythm Association (EHRA) registry of transvenous lead extraction outcomes. Eur Heart J 2017;38:2995–3005. - PubMed
-
- Sood N, Martin DT, Lampert R, Curtis JP, Parzynski C, Clancy J. Incidence and predictors of perioperative complications with transvenous lead extractions: real-world experience with National Cardiovascular Data Registry. Circ Arrhythm Electrophysiol 2018;11:e004768. - PubMed
-
- Polewczyk A, Rinaldi CA, Sohal M, Golzio P, Claridge S, Cano Oet al. . Transvenous lead extraction procedures in women based on ESC-EHRA EORP European Lead Extraction ConTRolled ELECTRa registry: is female sex a predictor of complications? Europace 2019;21:1890–9. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
