

Review
doi: 10.36660/abc.20220245.
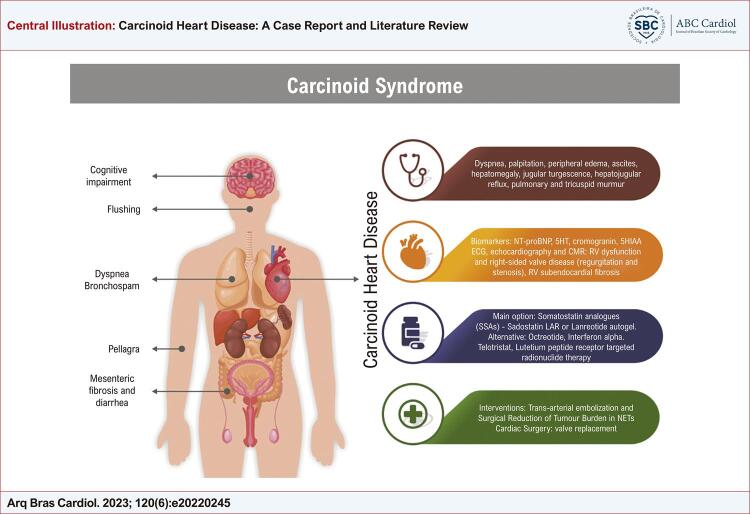
Carcinoid Heart Disease: A Case Report and Literature Review
[Article in
English,
Portuguese]
Affiliations
- PMID: 37466488
- PMCID: PMC10365021
- DOI: 10.36660/abc.20220245
Item in Clipboard
Review
Carcinoid Heart Disease: A Case Report and Literature Review
[Article in
English,
Portuguese]
Arq Bras Cardiol.
2023 Jun.
No abstract available
Conflict of interest statement
Potencial conflito de interesse
Não há conflito com o presente artigo
Figures
References
-
- 1. Mota JM, Sousa LG, Riechelmann RP. Complications from Carcinoid Syndrome: Review of the Current Evidence. Ecancermedicalscience. 2016;10:662. doi: 10.3332/ecancer.2016.662. - PMC - PubMed
- Mota JM, Sousa LG, Riechelmann RP. Complications from Carcinoid Syndrome: Review of the Current Evidence. 662Ecancermedicalscience. 2016;10 doi: 10.3332/ecancer.2016.662. - DOI - PMC - PubMed
-
- 2. Halperin DM, Shen C, Dasari A, Xu Y, Chu Y, Zhou S, et al. Frequency of Carcinoid Syndrome at Neuroendocrine Tumour Diagnosis: A Population-Based Study. Lancet Oncol. 2017;18(4):525-34. doi: 10.1016/S1470-2045(17)30110-9. - PMC - PubMed
- Halperin DM, Shen C, Dasari A, Xu Y, Chu Y, Zhou S, et al. Frequency of Carcinoid Syndrome at Neuroendocrine Tumour Diagnosis: A Population-Based Study. Lancet Oncol. 2017;18(4):525–534. doi: 10.1016/S1470-2045(17)30110-9. - DOI - PMC - PubMed
-
- 3. Ferrari ACRC, Glasberg J, Riechelmann RP. Carcinoid Syndrome: Update on the Pathophysiology and Treatment. Clinics. 2018;73(suppl 1):e490s. doi: 10.6061/clinics/2018/e490s. - PMC - PubMed
- Ferrari ACRC, Glasberg J, Riechelmann RP. Carcinoid Syndrome: Update on the Pathophysiology and Treatment. Clinics. 2018;73(suppl 1):e490s. doi: 10.6061/clinics/2018/e490s. - DOI - PMC - PubMed
-
- 4. Steeds R, Sagar V, Shetty S, Oelofse T, Singh H, Ahmad R, et al. Multidisciplinary Team Management of Carcinoid Heart Disease. Endocr Connect. 2019;8(12):R184-R199. doi: 10.1530/EC-19-0413. - PMC - PubMed
- Steeds R, Sagar V, Shetty S, Oelofse T, Singh H, Ahmad R, et al. Multidisciplinary Team Management of Carcinoid Heart Disease. Endocr Connect. 2019;8(12):R184–R199. doi: 10.1530/EC-19-0413. - DOI - PMC - PubMed
-
- 5. Pellikka PA, Tajik AJ, Khandheria BK, Seward JB, Callahan JA, Pitot HC, et al. Carcinoid Heart Disease. Clinical and Echocardiographic Spectrum in 74 Patients. Circulation. 1993;87(4):1188-96. doi: 10.1161/01.cir.87.4.1188. - PubMed
- Pellikka PA, Tajik AJ, Khandheria BK, Seward JB, Callahan JA, Pitot HC, et al. Carcinoid Heart Disease. Clinical and Echocardiographic Spectrum in 74 Patients. Circulation. 1993;87(4):1188–1196. doi: 10.1161/01.cir.87.4.1188. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
