

Understanding a mass in the paraspinal region: an anatomical approach
- PMID: 37466751
- PMCID: PMC10356722
- DOI: 10.1186/s13244-023-01462-1
Understanding a mass in the paraspinal region: an anatomical approach
Abstract
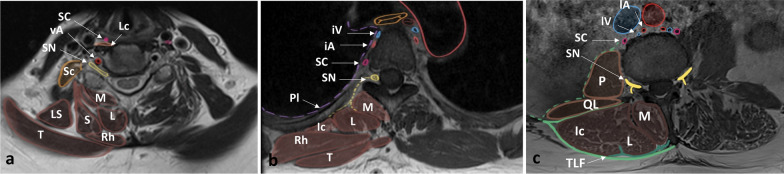
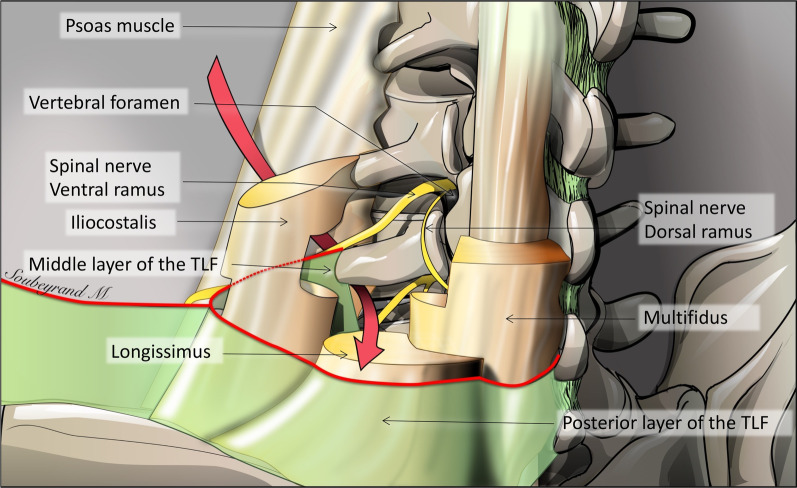
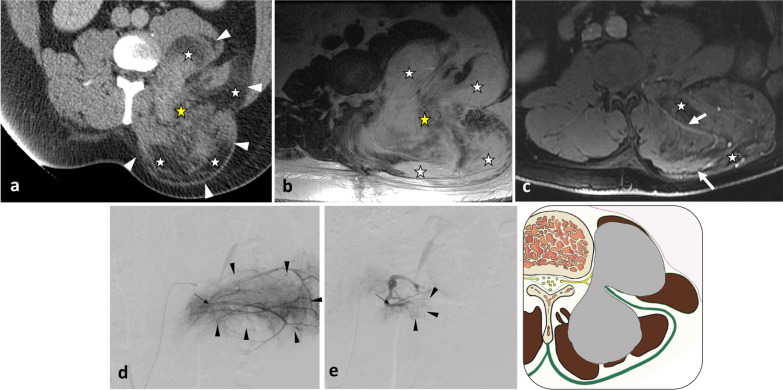
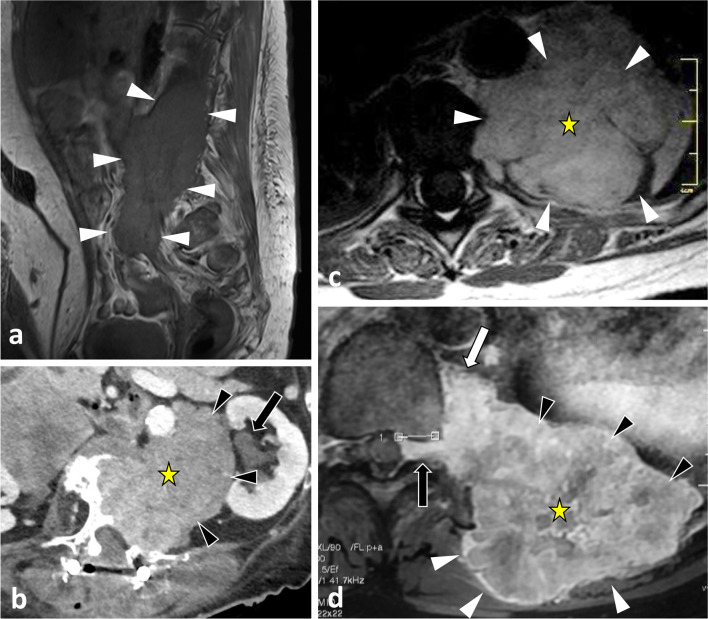
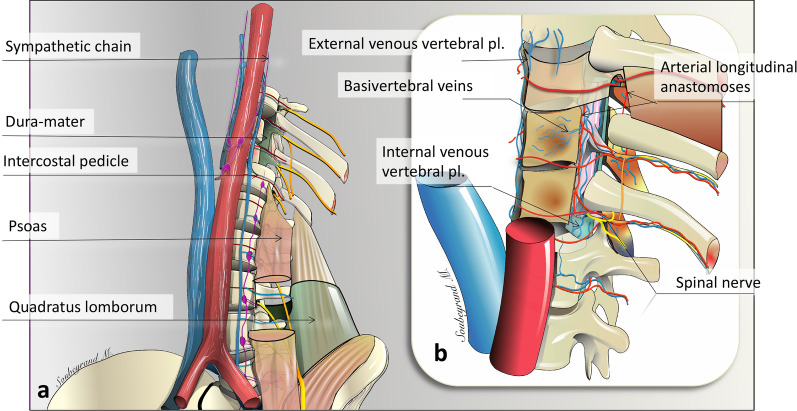
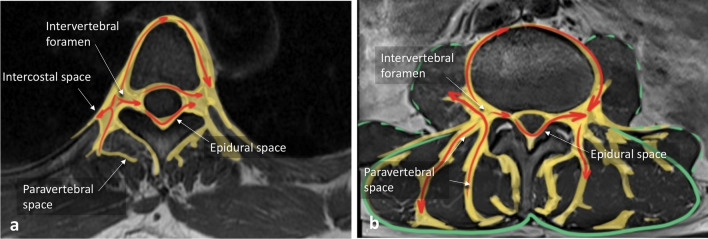
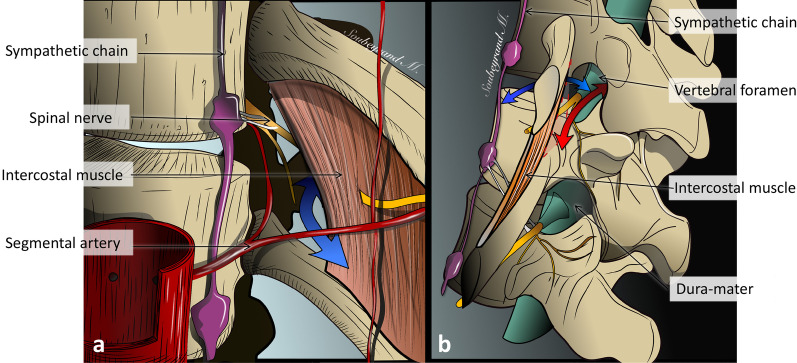
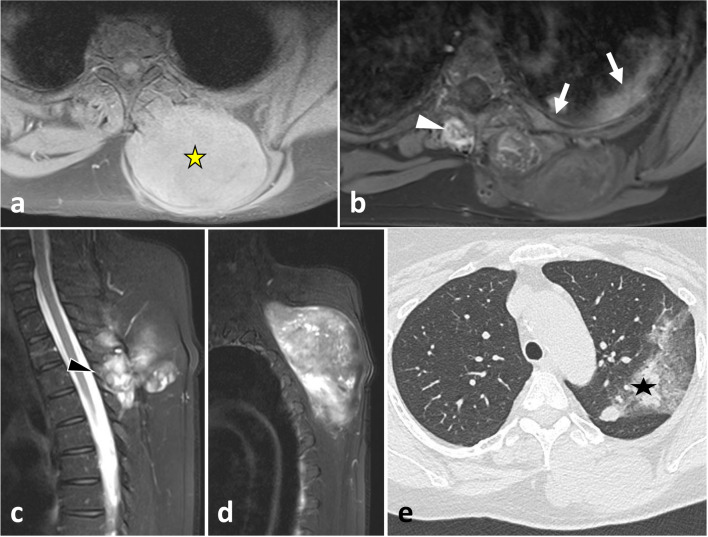
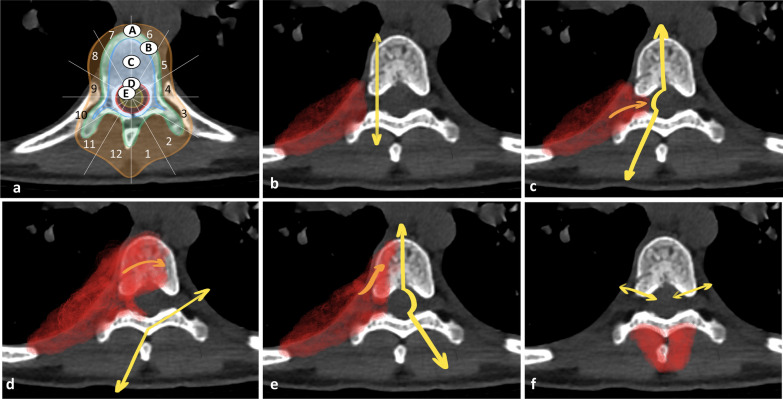
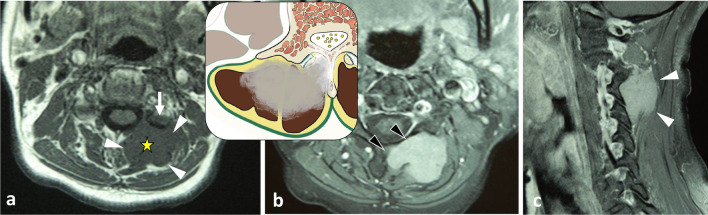
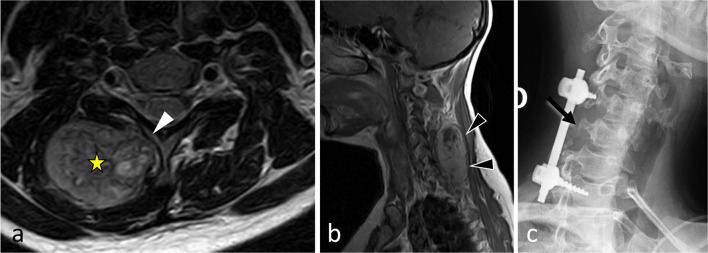
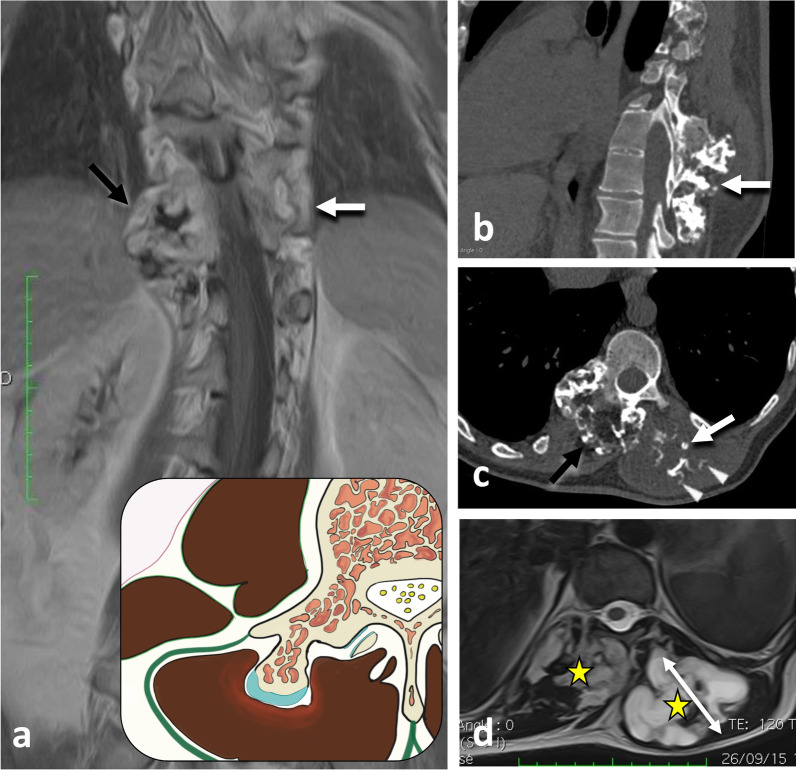
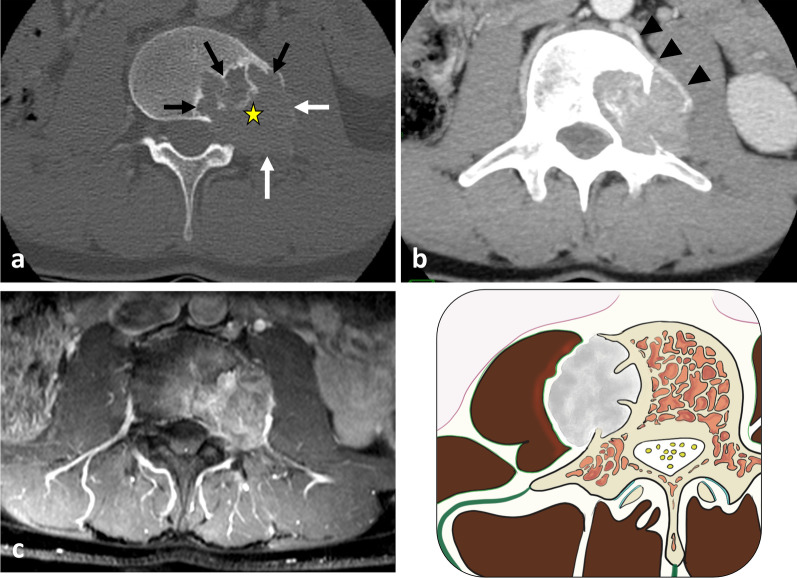
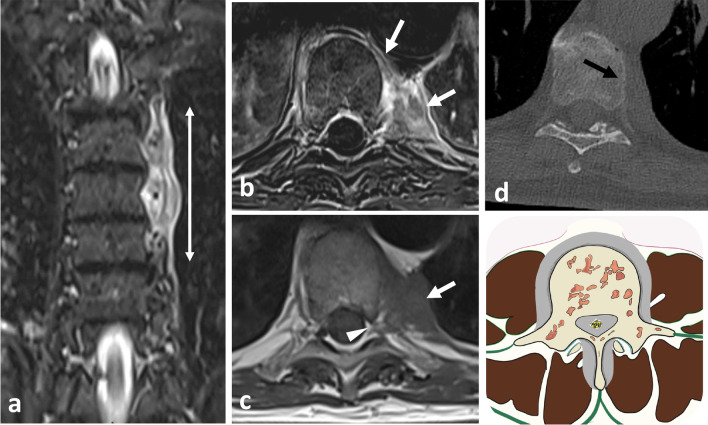
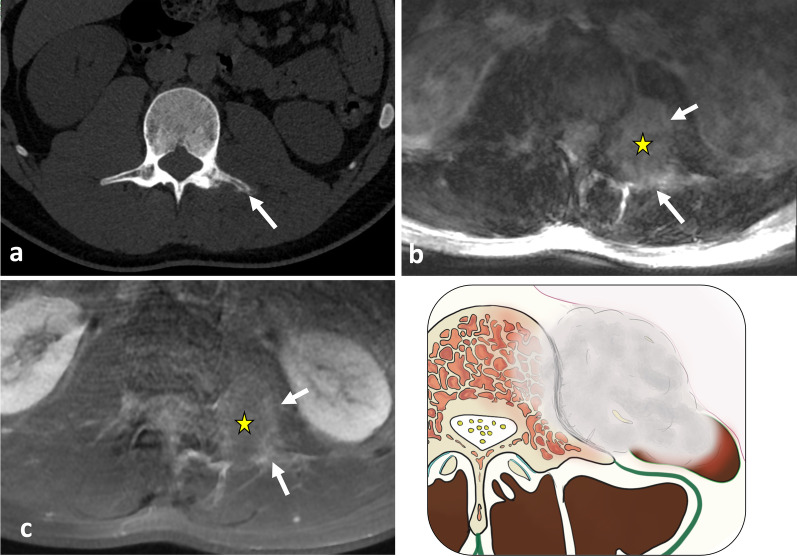
The paraspinal region encompasses all tissues around the spine. The regional anatomy is complex and includes the paraspinal muscles, spinal nerves, sympathetic chains, Batson's venous plexus and a rich arterial network. A wide variety of pathologies can occur in the paraspinal region, originating either from paraspinal soft tissues or the vertebral column. The most common paraspinal benign neoplasms include lipomas, fibroblastic tumours and benign peripheral nerve sheath tumours. Tumour-like masses such as haematomas, extramedullary haematopoiesis or abscesses should be considered in patients with suggestive medical histories. Malignant neoplasms are less frequent than benign processes and include liposarcomas and undifferentiated sarcomas. Secondary and primary spinal tumours may present as midline expansile soft tissue masses invading the adjacent paraspinal region. Knowledge of the anatomy of the paraspinal region is of major importance since it allows understanding of the complex locoregional tumour spread that can occur via many adipose corridors, haematogenous pathways and direct contact. Paraspinal tumours can extend into other anatomical regions, such as the retroperitoneum, pleura, posterior mediastinum, intercostal space or extradural neural axis compartment. Imaging plays a crucial role in formulating a hypothesis regarding the aetiology of the mass and tumour staging, which informs preoperative planning. Understanding the complex relationship between the different elements and the imaging features of common paraspinal masses is fundamental to achieving a correct diagnosis and adequate patient management. This review gives an overview of the anatomy of the paraspinal region and describes imaging features of the main tumours and tumour-like lesions that occur in the region.
Keywords: Anatomy; Imaging; Paraspinal muscle; Soft tissue neoplasm; Spinal neoplasm.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
-
- Jorgensen K. Human trunk extensor muscles physiology and ergonomics. Acta Physiol Scand Suppl. 1997;637:1–58. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
