

Individual Participant Data Network Meta-Analysis of Neoadjuvant Chemotherapy or Chemoradiotherapy in Esophageal or Gastroesophageal Junction Carcinoma
- PMID: 37467395
- PMCID: PMC10553121
- DOI: 10.1200/JCO.22.02279
Individual Participant Data Network Meta-Analysis of Neoadjuvant Chemotherapy or Chemoradiotherapy in Esophageal or Gastroesophageal Junction Carcinoma
Abstract
Purpose: The optimal neoadjuvant treatment for resectable carcinoma of the thoracic esophagus (TE) or gastroesophageal junction (GEJ) remains a matter of debate. We performed an individual participant data (IPD) network meta-analysis (NMA) of randomized controlled trials (RCTs) to study the effect of chemotherapy or chemoradiotherapy, with a focus on tumor location and histology subgroups.
Patients and methods: All, published or unpublished, RCTs closed to accrual before December 31, 2015 and having compared at least two of the following strategies were eligible: upfront surgery (S), chemotherapy followed by surgery (CS), and chemoradiotherapy followed by surgery (CRS). All analyses were conducted on IPD obtained from investigators. The primary end point was overall survival (OS). The IPD-NMA was analyzed by a one-step mixed-effect Cox model adjusted for age, sex, tumor location, and histology. The NMA was registered in PROSPERO (CRD42018107158).
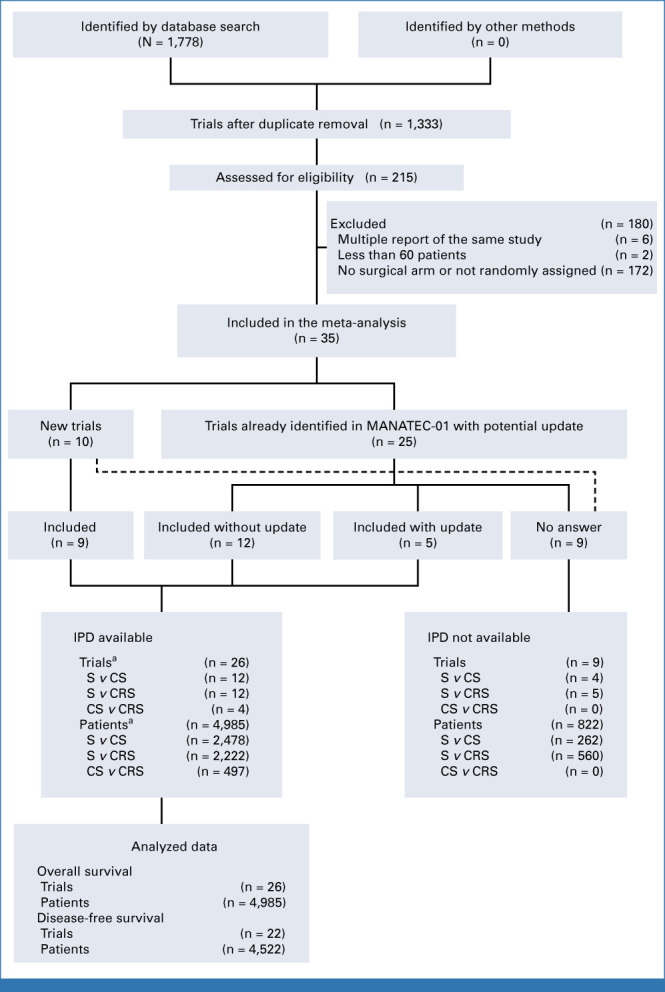
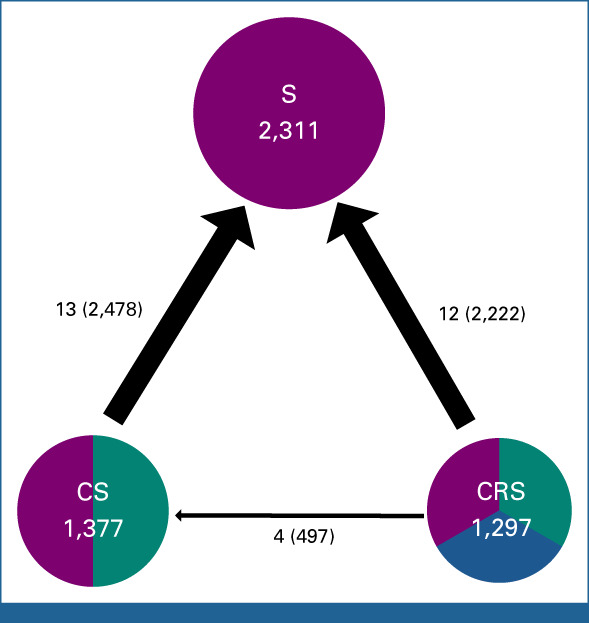
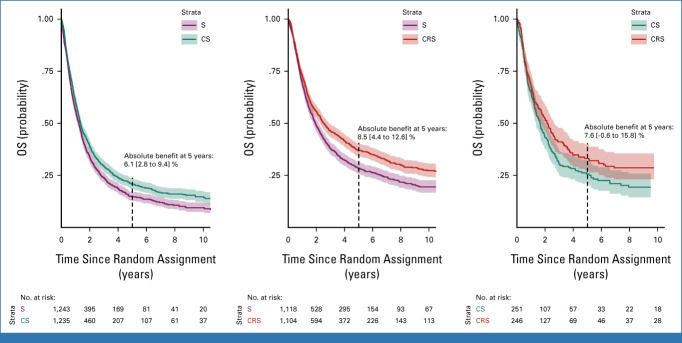
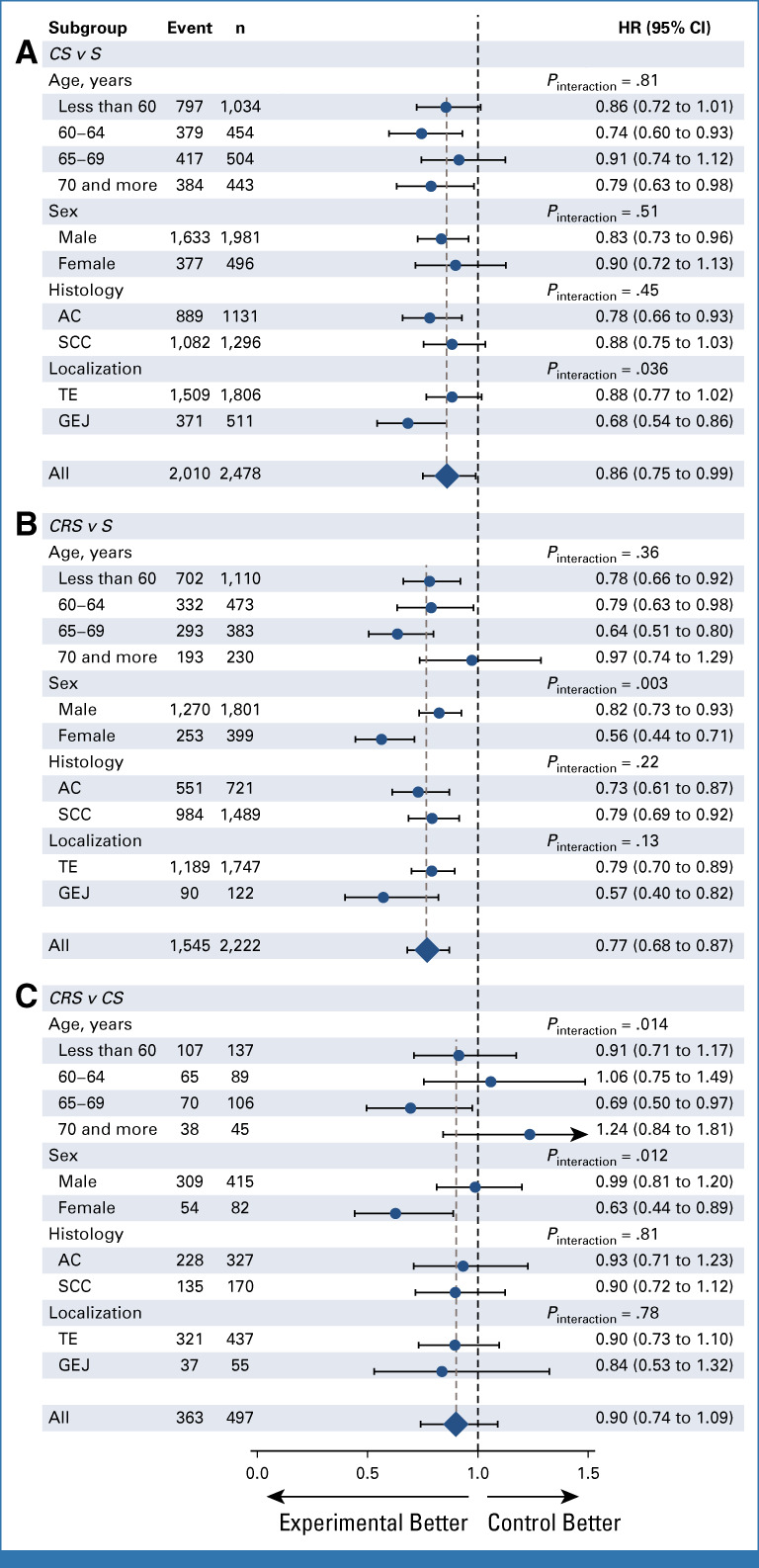
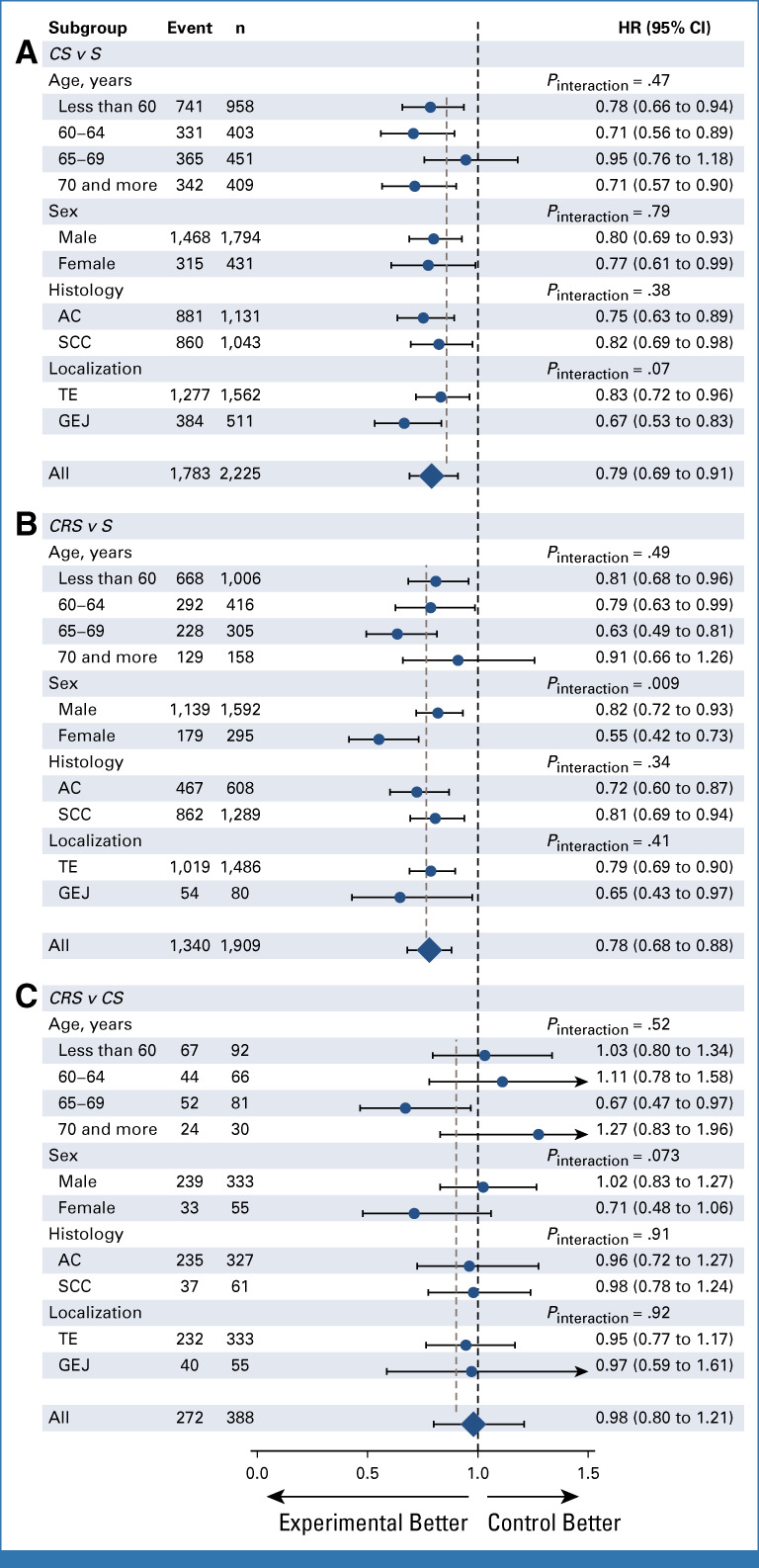
Results: IPD were obtained for 26 of 35 RCTs (4,985 of 5,807 patients) corresponding to 12 comparisons for CS-S, 12 for CRS-S, and four for CRS-CS. CS and CRS led to increased OS when compared with S with hazard ratio (HR) = 0.86 (0.75 to 0.99), P = .03 and HR = 0.77 (0.68 to 0.87), P < .001 respectively. The NMA comparison of CRS versus CS for OS gave a HR of 0.90 (0.74 to 1.09), P = .27 (consistency P = .26, heterogeneity P = .0038). For CS versus S, a larger effect on OS was observed for GEJ versus TE tumors (P = .036). For the CRS versus S and CRS versus CS, a larger effect on OS was observed for women (P = .003, .012, respectively).
Conclusion: Neoadjuvant chemotherapy and chemoradiotherapy were consistently better than S alone across histology, but with some variation in the magnitude of treatment effect by sex for CRS and tumor location for CS. A strong OS difference between CS and CRS was not identified.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
References
-
- World Health Organization . GLOBOCAN—Cancer Today. 2020. http://gco.iarc.fr/today/home
-
- Obermannová R, Alsina M, Cervantes A, et al. : Oesophageal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol 33:992-1004, 2022 - PubMed
-
- National Comprehensive Cancer Network : Esophageal and Esophagogastric Junction Cancers. NCCN. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1433 - PubMed
-
- Faron M, Cheugoua-Zanetsie AM, Thirion P, et al. : Individual patient data meta-analysis of neoadjuvant chemotherapy followed by surgery versus upfront surgery for carcinoma of the oesophagus or the gastro-oesophageal junction. Eur J Cancer 157:278-290, 2021 - PubMed
-
- Ronellenfitsch U, Schwarzbach M, Hofheinz R, et al. : Preoperative chemo(radio)therapy versus primary surgery for gastroesophageal adenocarcinoma: Systematic review with meta-analysis combining individual patient and aggregate data. Eur J Cancer 49:3149-3158, 2013 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
