

Phase II Study of Olaparib and Temozolomide for Advanced Uterine Leiomyosarcoma (NCI Protocol 10250)
- PMID: 37467452
- PMCID: PMC10852403
- DOI: 10.1200/JCO.23.00402
Phase II Study of Olaparib and Temozolomide for Advanced Uterine Leiomyosarcoma (NCI Protocol 10250)
Erratum in
-
Erratum: Phase II Study of Olaparib and Temozolomide for Advanced Uterine Leiomyosarcoma (NCI Protocol 10250).J Clin Oncol. 2023 Nov 20;41(33):5205. doi: 10.1200/JCO.23.02063. Epub 2023 Oct 6. J Clin Oncol. 2023. PMID: 37801676 No abstract available.
Abstract
Purpose: Uterine leiomyosarcoma (uLMS) is an aggressive subtype of soft-tissue sarcoma with frequent metastatic relapse after curative surgery. Chemotherapy provides limited benefit for advanced disease. Multiomics profiling studies have identified homologous recombination deficiency in uLMS. In preclinical studies where olaparib and temozolomide provided modest activity, the combination was highly effective for inhibiting uLMS tumor growth.
Patients and methods: NCI Protocol 10250 is a single-arm, open-label, multicenter, phase II study evaluating olaparib and temozolomide in advanced uLMS. Patients with progression on ≥1 prior line received temozolomide 75 mg/m2 orally once daily with olaparib 200 mg orally twice a day both on days 1-7 in 21-day cycles. The primary end point was the best objective response rate (ORR) within 6 months. A one-stage binomial design was used. If ≥5 of 22 responded, the treatment would be considered promising (93% power; α = .06). All patients underwent paired biopsies that were evaluated with whole-exome sequencing (WES)/RNAseq and a RAD51 foci formation assay.
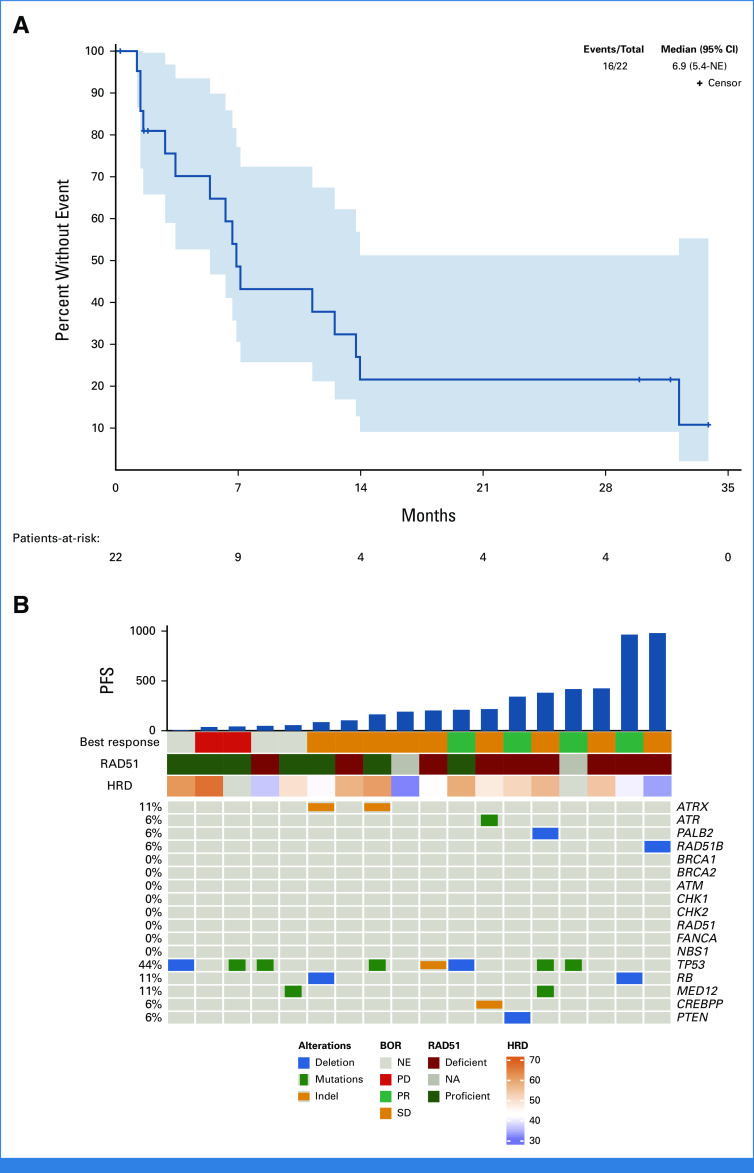
Results: Twenty-two patients were evaluable. The median age was 55 years, and 59% had received three or more prior lines. Best ORR within 6 months was 23% (5 of 22). The overall ORR was 27% (6 of 22). The median progression-free survival (mPFS) was 6.9 months (95% CI, 5.4 months to not estimable). Hematologic toxicity was common (grade 3/4 neutropenia: 75%; thrombocytopenia: 32%) but manageable with dose modification. Five of 16 (31%) of tumors contained a deleterious homologous recombination gene alteration by WES, and 9 of 18 (50%) were homologous recombination-deficient by the RAD51 assay. In an exploratory analysis, mPFS was prolonged for patients with homologous recombination-deficient versus homologous recombination-proficient tumors (11.2 v 5.4 months, P = .05) by RAD51.
Conclusion: Olaparib and temozolomide met the prespecified primary end point and provided meaningful clinical benefit in patients with advanced, pretreated uLMS.
Trial registration: ClinicalTrials.gov NCT03880019.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures







References
-
- Gadducci A, Landoni F, Sartori E, et al. Uterine leiomyosarcoma: Analysis of treatment failures and survival. Gynecol Oncol. 1996;62:25–32. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
