

Prescription Opioid Initiation for Neuropathy, Headache, and Low Back Pain: A US Population-based Medicare Study
- PMID: 37468023
- PMCID: PMC11529292
- DOI: 10.1016/j.jpain.2023.07.011
Prescription Opioid Initiation for Neuropathy, Headache, and Low Back Pain: A US Population-based Medicare Study
Abstract
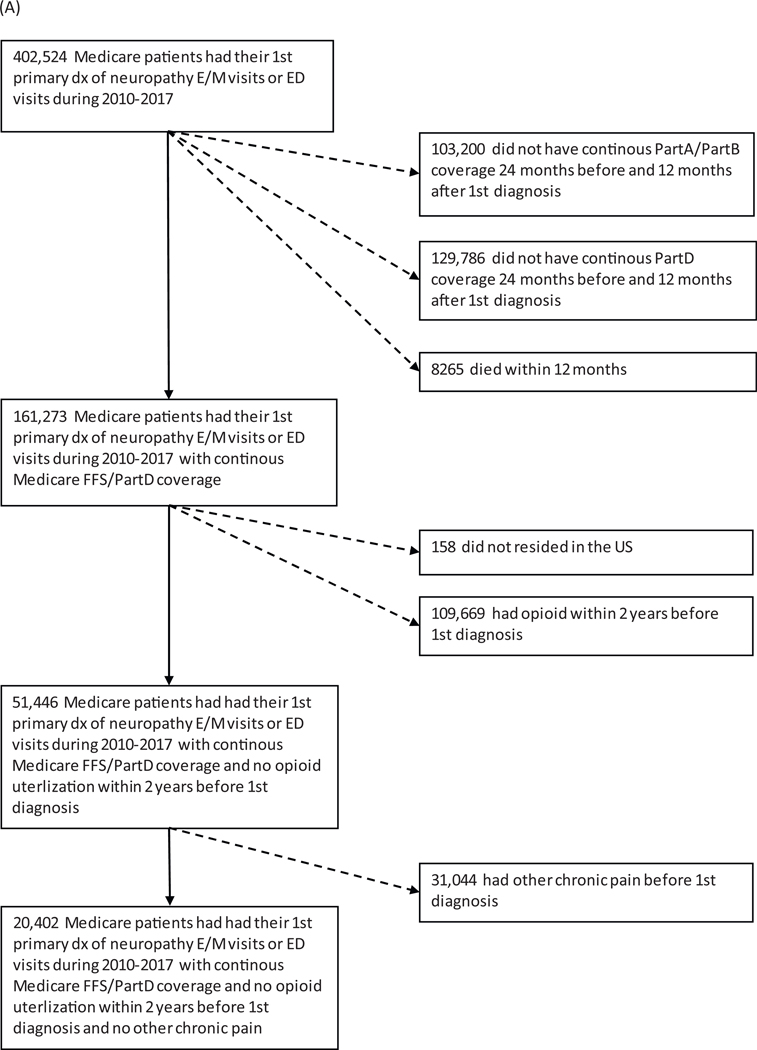
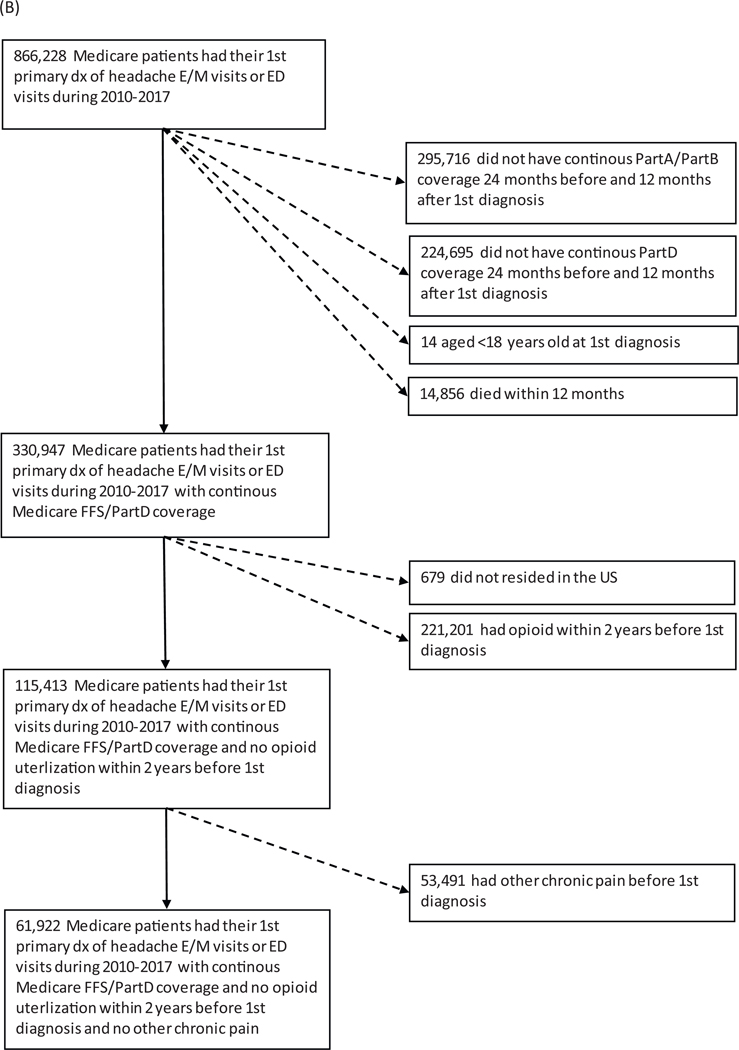
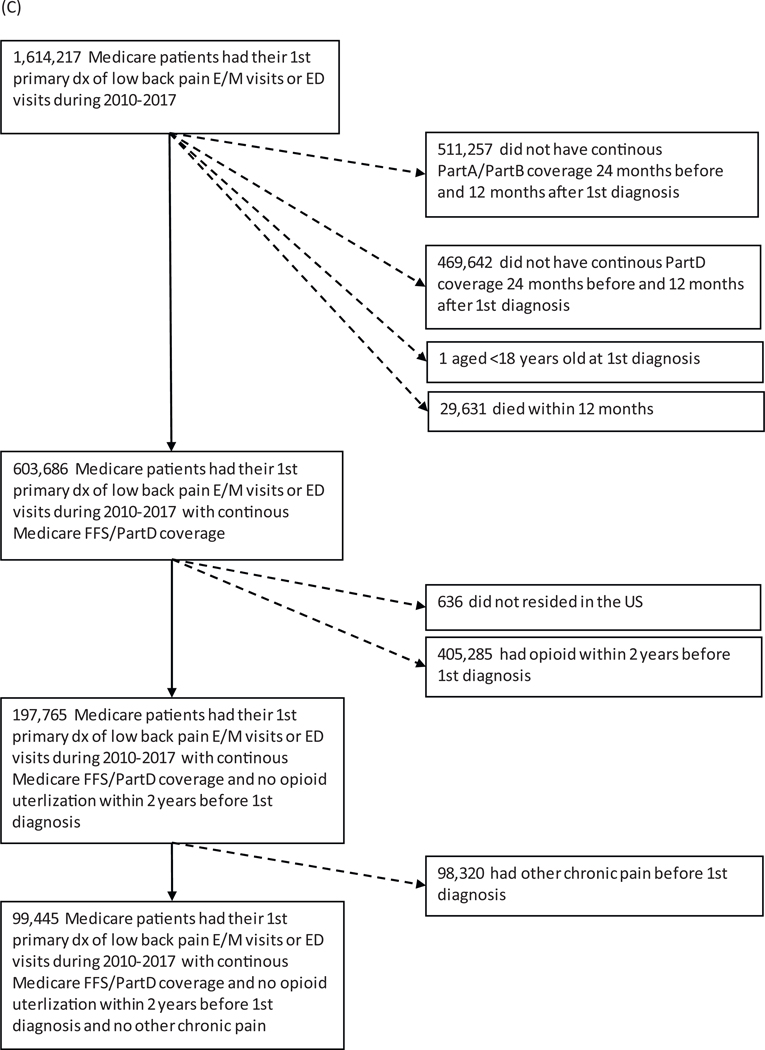
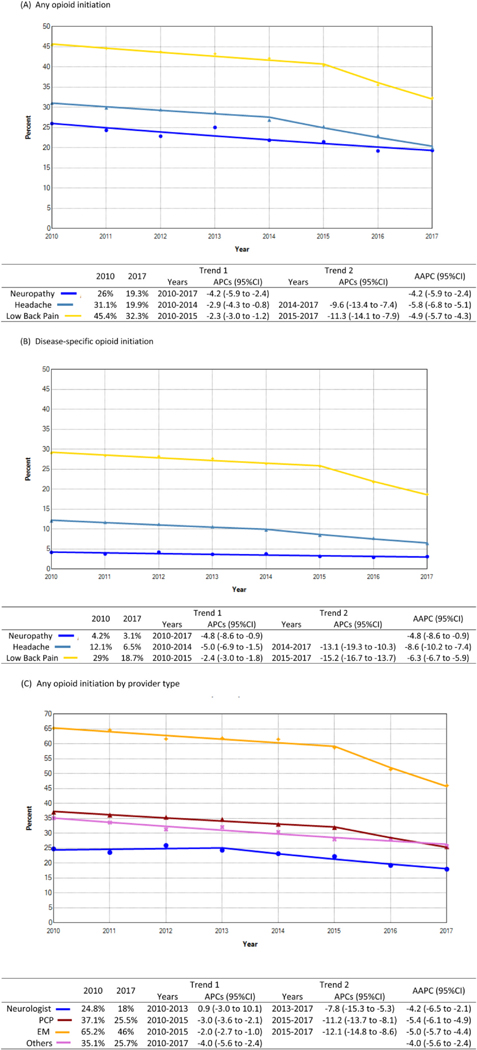
Neuropathy, headache, and low back pain (LBP) are common conditions requiring pain management. Yet little is known regarding whether access to specialists impacts opioid prescribing. We aimed to identify factors associated with opioid initiation among opioid-naïve older adults and evaluate how access to particular specialists impacts prescribing. This retrospective cohort study used a 20% Medicare sample from 2010 to 2017. Opioid initiation was defined as a first opioid prescription filled within 12 months after a diagnosis encounter. Disease-related opioid initiation was defined as a first opioid prescription filled within 7 days following a disease-specific claim. Logistic regression using generalized estimating equations was used to determine the association of patient demographics, provider types, and regional physician specialty density with disease-related opioid initiation, accounting for within-region correlation. We found opioid initiation steadily declined from 2010 to 2017 (neuropathy: 26-19%, headache: 31-20%, LBP: 45-32%), as did disease-related opioid initiation (4-3%, 12-7%, 29-19%) and 5 to 10% of initial disease-related prescriptions resulted in chronic opioid use within 12 months of initiation. Certain specialist visits were associated with a lower likelihood of disease-related opioid initiation compared with primary care. Residence in high neurologist density regions had a lower likelihood of disease-related opioid initiation (headache odds ratio [OR] .76 [95% CI: .63-.92]) and LBP (OR .7 [95% CI: .61-.81]) and high podiatrist density regions for neuropathy (OR .56 [95% CI: .41-.78]). We found that specialist visits and greater access to specialists were associated with a lower likelihood of disease-related opioid initiation. These data could inform strategies to perpetuate reductions in opioid use for these common pain conditions. PERSPECTIVE: This article presents how opioid initiation for opioid-naïve patients with newly diagnosed neuropathy, headache, and LBP varies across providers. Greater access to certain specialists decreased the likelihood of opioid initiation. Future work may consider interventions to support alternative treatments and better access to specialists in low-density regions.
Keywords: Medicare; Opioids; access to specialists; geographic variation; prescribing.
Copyright © 2023 United States Association for the Study of Pain, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Observational retrospective study of the association of initial healthcare provider for new-onset low back pain with early and long-term opioid use.BMJ Open. 2019 Sep 20;9(9):e028633. doi: 10.1136/bmjopen-2018-028633. BMJ Open. 2019. PMID: 31542740 Free PMC article.
-
Opioid Use in Adults With Low Back or Lower Extremity Pain Who Undergo Spine Surgical Treatment Within 1 Year of Diagnosis.Spine (Phila Pa 1976). 2020 Dec 15;45(24):1725-1735. doi: 10.1097/BRS.0000000000003663. Spine (Phila Pa 1976). 2020. PMID: 32833930
-
The association between the supply of select nonpharmacologic providers for pain and use of nonpharmacologic pain management services and initial opioid prescribing patterns for Medicare beneficiaries with persistent musculoskeletal pain.Health Serv Res. 2021 Apr;56(2):275-288. doi: 10.1111/1475-6773.13561. Epub 2020 Oct 1. Health Serv Res. 2021. PMID: 33006158 Free PMC article.
-
Opioids for low back pain.BMJ. 2015 Jan 5;350:g6380. doi: 10.1136/bmj.g6380. BMJ. 2015. PMID: 25561513 Free PMC article. Review.
-
Harms and benefits of opioids for management of non-surgical acute and chronic low back pain: a systematic review.Br J Sports Med. 2020 Jun;54(11):664. doi: 10.1136/bjsports-2018-099805. Epub 2019 Mar 22. Br J Sports Med. 2020. PMID: 30902816
Cited by
-
Association of Opioid Use Disorder Diagnosis with Management of Acute Low Back Pain: A Medicare Retrospective Cohort Analysis.J Gen Intern Med. 2024 Aug;39(11):2097-2105. doi: 10.1007/s11606-024-08799-3. Epub 2024 Jun 3. J Gen Intern Med. 2024. PMID: 38829451 Free PMC article.
References
-
- National Center for Injury PCDoUIP: Clinical evidence review for the CDC guideline for prescribing opioids for chronic pain – United States, 2016. MMWR Recommend Rep 65:1–49, 2016 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
