

Estimating long-term vaccine effectiveness against SARS-CoV-2 variants: a model-based approach
- PMID: 37468463
- PMCID: PMC10356855
- DOI: 10.1038/s41467-023-39736-3
Estimating long-term vaccine effectiveness against SARS-CoV-2 variants: a model-based approach
Abstract
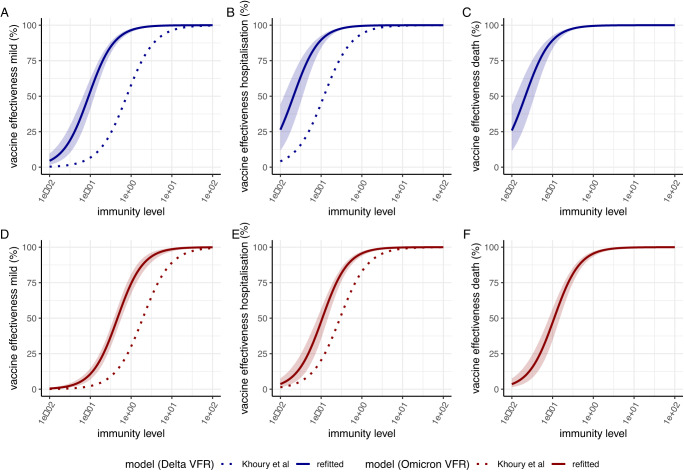
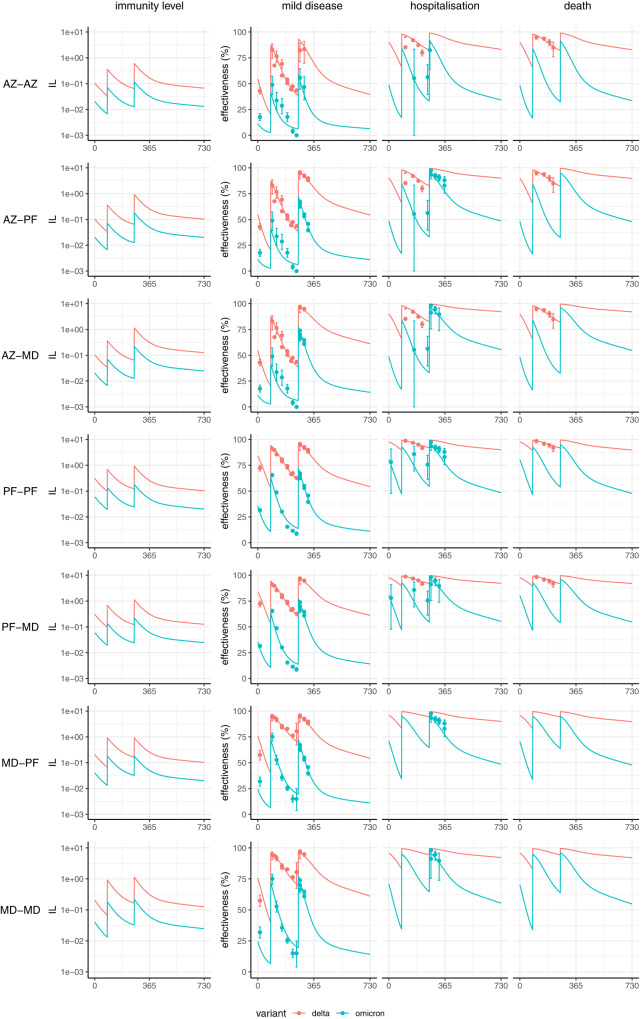
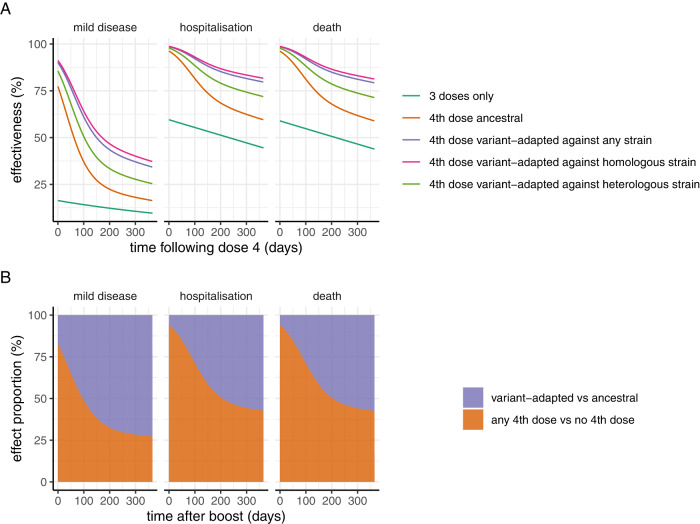
With the ongoing evolution of the SARS-CoV-2 virus updated vaccines may be needed. We fitted a model linking immunity levels and protection to vaccine effectiveness data from England for three vaccines (Oxford/AstraZeneca AZD1222, Pfizer-BioNTech BNT162b2, Moderna mRNA-1273) and two variants (Delta, Omicron). Our model reproduces the observed sustained protection against hospitalisation and death from the Omicron variant over the first six months following dose 3 with the ancestral vaccines but projects a gradual waning to moderate protection after 1 year. Switching the fourth dose to a variant-matched vaccine against Omicron BA.1/2 is projected to prevent nearly twice as many hospitalisations and deaths over a 1-year period compared to administering the ancestral vaccine. This result is sensitive to the degree to which immunogenicity data can be used to predict vaccine effectiveness and uncertainty regarding the impact that infection-induced immunity (not captured here) may play in modifying future vaccine effectiveness.
© 2023. The Author(s).
Conflict of interest statement
A.C.G. has participated as a non-renumerated member of a scientific advisory board for Moderna, has received consultancy funding from GSK and Sanofi for activities related to COVID-19 vaccination and is a member of the CEPI scientific advisory board and Gavi Vaccine Investment Strategy steering committee. She has received grant funding from Gavi for COVID-19-related work. A.B.H., P.W. and A.C.G. have previously received consultancy payments from WHO for COVID-19-related work. ABH provides COVID-19 modelling advice to the New South Wales Ministry of Health, Australia. A.B.H. was previously engaged by Pfizer Inc to advise on modelling RSV vaccination strategies for which she received no financial compensation. E.M.R. is a non-remunerated member of the UK Vaccines Network, the UKRI COVID-19 taskforce and the British Society for Immunology Covid-19 taskforce. The remaining authors declare no competing interests.
Figures
References
-
- Schneider, E. C. et al. The U. S. COVID-19 vaccination program at one year: how many deaths and hospitalizations were averted? Commonwealth Fund. https://www.commonwealthfund.org/publications/issue-briefs/2021/dec/us-c... (2021).
-
- Singanayagam A, et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study. Lancet Infect. Dis. 2022;22:183–195. doi: 10.1016/S1473-3099(21)00648-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
