

Immune response to pertussis vaccine in COPD patients
- PMID: 37468500
- PMCID: PMC10356756
- DOI: 10.1038/s41598-023-38355-8
Immune response to pertussis vaccine in COPD patients
Abstract
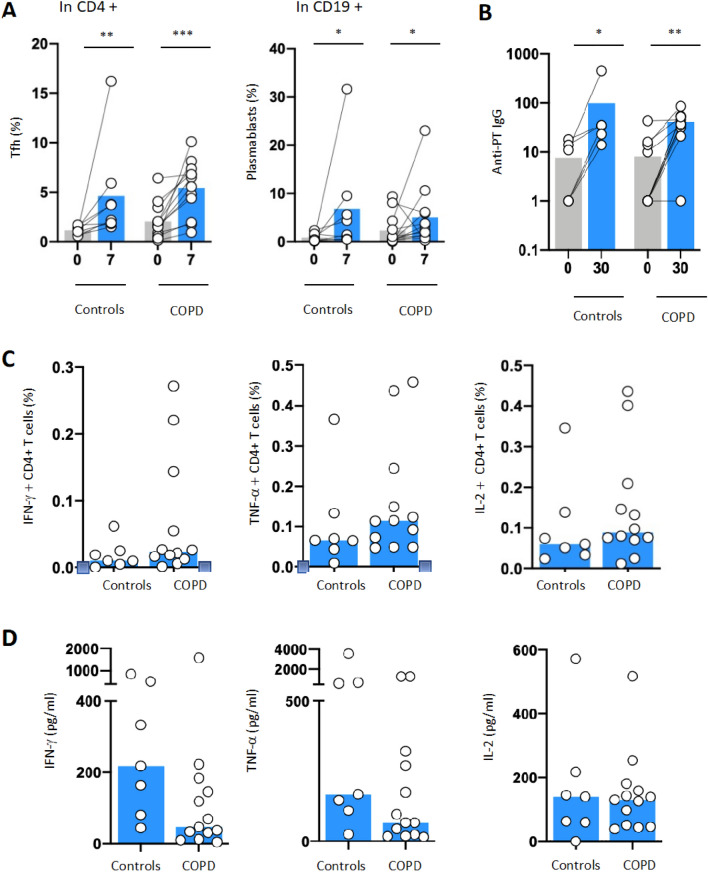
Exacerbation triggered by respiratory infection is an important cause of morbidity and mortality in chronic obstructive pulmonary disease (COPD) patients. Strategies aiming to preventing infection may have significant public health impact. Our previous study demonstrated decreased immunological response to seasonal flu vaccination in COPD patients, questioning the efficiency of other vaccines in this group of patients. We performed a prospective, monocenter, longitudinal study that evaluated the humoral and cellular responses upon pertussis vaccination. We included 13 patients with stable COPD and 8 healthy volunteers. No difference in circulating B and T cell subsets at baseline was noted. Both groups presented similar levels of TFH, plasmablasts and pertussis specific antibodies induction after vaccination. Moreover, monitoring T cell immunity after ex-vivo peptide stimulation revealed equivalent induction of functional and specific CD4+ T cells (IFNγ, TNFα and IL-2-expressing T cells) in both groups. Our results highlight the immunological efficiency of pertussis vaccination in this particularly vulnerable population and challenge the concept that COPD patients are less responsive to all immunization strategies. Healthcare providers should stress the necessity of decennial Tdap booster vaccination in COPD patients.
© 2023. The Author(s).
Conflict of interest statement
C.C has consultant arrangements and has received grants from Astra Zeneca, Boehringer Ingelheim, MSD, Pierre Fabre Oncology, Lilly, Roche, Bristol Myers Squibb, and Novartis. J.D.L has board membership with IVIR-AC Comitee WHO, Member of the French NITAG, Work package leader VRI (HIV vaccine-France), Work package leader EHVA project (HIV vaccine-EU), Work package leader Vaccelerate project (COVID19 vaccine-EU). The rest of the authors declare that they have no relevant conflicts of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
