

A novel and superior Lasso-plate technique in treatment for coronoid process fracture in the terrible triad of elbow
- PMID: 37468520
- PMCID: PMC10356941
- DOI: 10.1038/s41598-023-38885-1
A novel and superior Lasso-plate technique in treatment for coronoid process fracture in the terrible triad of elbow
Abstract
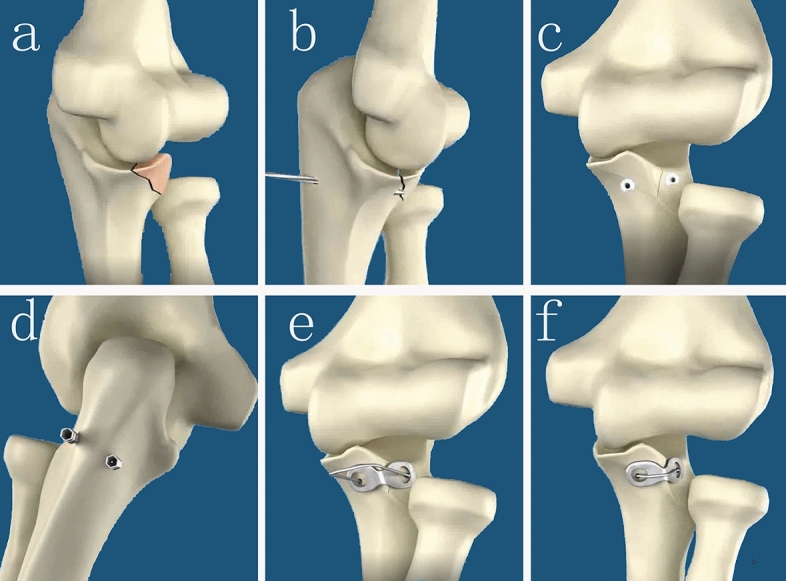
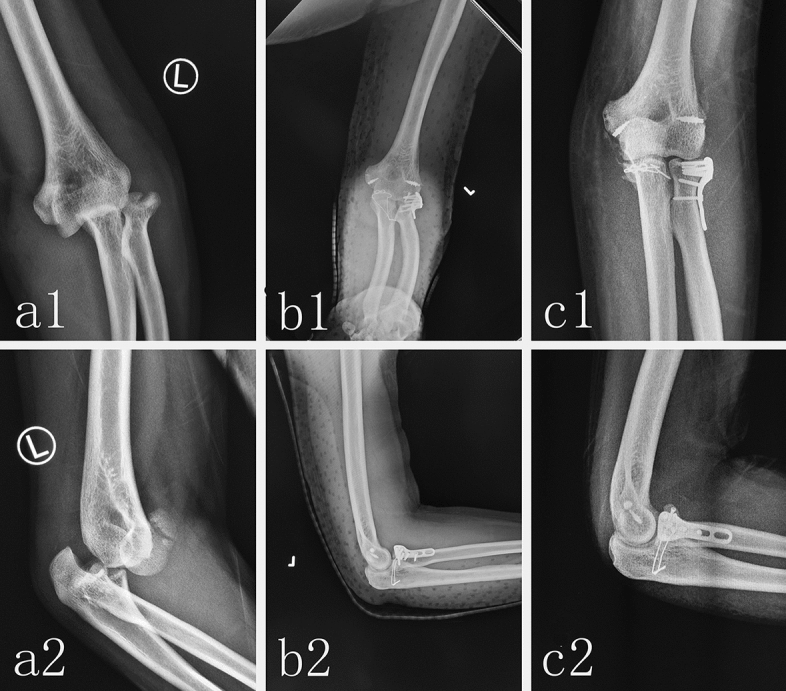
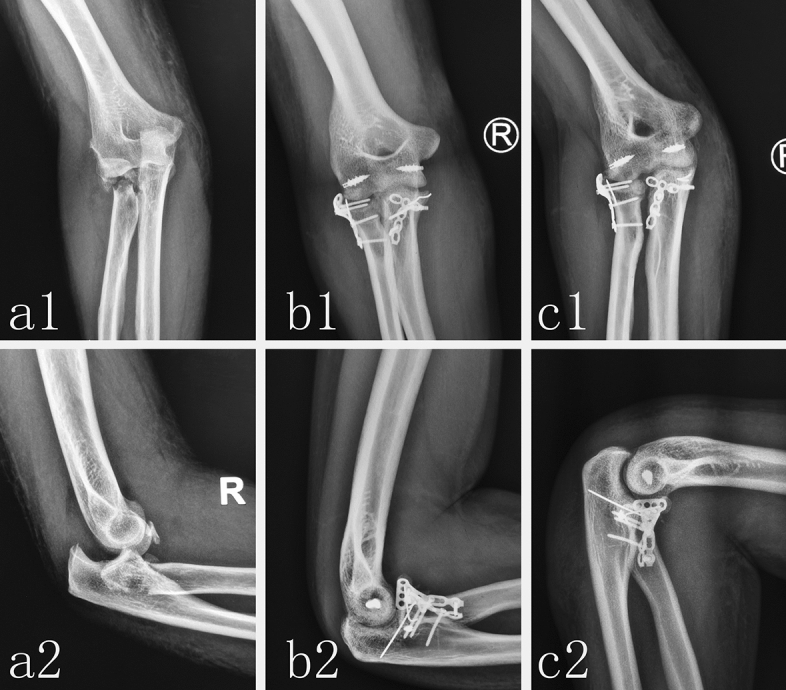
The treatment of ulna coronal process fractures in the terrible triad of elbow, especially type I and II Regan-Morrey coronoid fractures, still have been controversial. The purpose of this retrospective study was to evaluate the novel Lasso-plate technique to have a more reliable fixation and a well clinical outcomes for type I and II Regan-Morrey coronoid fractures in a terrible triad of the elbow (TTE). Patients with simple TTE, closed fracture, aged > 18 years, duration of injury < 2 weeks, type I and II Regan-Morrey coronoid process fracture fixed by the Lasso-plate technique or ORIF were enrolled in the study. Total 144 patients with type I and II Regan-Morrey coronoid fracture in TTE were included in the Lasso-plate group or ORIF (open reduction and internal fixation) group in the Xi'an Honghui Hospital from January 2017 to December 2020. Eighty-six patients in Lasso-plate group underwent surgery using a novel Lasso-plate technique. And other 58 patients in ORIF group underwent surgery using ORIF. The data of two groups, including the X-ray films, Computed tomography (CT), the range of elbow motion, Mayo Elbow Performance Score (MEPS) and the surgical complications, were extracted from the hospital's patient records. All patients in both groups were followed up at least 12 months. The mean operation time (88.2 ± 12.3 min) in Lasso-plate group is shorter than that of ORIF group (109.1 ± 13.0 min). There was one patient with injury of deep branch of radial nerve and one patient with superficial surgical incision infection in Lasso-plate group. There were two patients with surgical incision infection in ORIF group. There were three heterotopic ossifications in Lasso-plate group and eight heterotopic ossifications in ORIF group. There were 5 elbow joints stiffness in Lasso-plate group and 12 in ORIF group. At 12 months follow up, the mean range of flexion-extension motion in Lasso-plate group was 122.9° ± 13.4° versus 113.2° ± 18.1° in ORIF group (p < 0.01), the mean 89.7 ± 5.6 MEPS in Lasso-plate group versus mean 83.7 ± 6.1 MEPSin ORIF group. The fixation of coronoid process fracture in TTE by the Lasso-plate technique, especially type I and II Regan-Morrey coronoid fracture, could be easier to master and operate, could provide the sufficient stability of elbow joint to enable early functional exercise, along with a better clinical outcome, a lower surgical complication. For the treatment of TTE, we recommend the fixation of type I and II Regan-Morrey coronoid fracture with the Lasso-plate technique, which would result in a better clinical outcome.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Lasso plate - An original implant for fixation of type I and II Regan-Morrey coronoid fractures.Orthop Traumatol Surg Res. 2017 May;103(3):447-451. doi: 10.1016/j.otsr.2016.12.017. Epub 2017 Feb 7. Orthop Traumatol Surg Res. 2017. PMID: 28185992
-
Terrible triad injuries of the elbow: does the coronoid always need to be fixed?Clin Orthop Relat Res. 2014 Jul;472(7):2084-91. doi: 10.1007/s11999-014-3471-7. Clin Orthop Relat Res. 2014. PMID: 24474322 Free PMC article.
-
[Extensor digitorum communis split approach combined with loop-plate technique for treatment of ulnar coronoid fracture in terrible triad of elbow].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021 Apr 15;35(4):420-425. doi: 10.7507/1002-1892.202010081. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021. PMID: 33855824 Free PMC article. Chinese.
-
Plate fixation through an anterior approach for coronoid process fractures: A retrospective case series and a literature review.Medicine (Baltimore). 2018 Sep;97(36):e12041. doi: 10.1097/MD.0000000000012041. Medicine (Baltimore). 2018. PMID: 30200084 Free PMC article. Review.
-
Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. Surgical technique.J Bone Joint Surg Am. 2005 Mar;87 Suppl 1(Pt 1):22-32. doi: 10.2106/JBJS.D.02933. J Bone Joint Surg Am. 2005. PMID: 15743844 Review.
Cited by
-
Arthroscopic Reduction and Transosseous Fixation of the Elbow Coronoid Process Fracture Using High-Strength Suture.Arthrosc Tech. 2025 Jan 27;14(4):103341. doi: 10.1016/j.eats.2024.103341. eCollection 2025 Apr. Arthrosc Tech. 2025. PMID: 40452990 Free PMC article.
References
-
- Hotchkiss RN. Fractures and dislocations of the elbow. In: Rockwood CA, Green DP, Bucholz RW, editors. Rockwood and Green’s Fractures in Adults. 4. Lippincott Raven; 1996. pp. 929–1024.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
