

Measuring acute effects of subanesthetic ketamine on cerebrovascular hemodynamics in humans using TD-fNIRS
- PMID: 37468572
- PMCID: PMC10356754
- DOI: 10.1038/s41598-023-38258-8
Measuring acute effects of subanesthetic ketamine on cerebrovascular hemodynamics in humans using TD-fNIRS
Abstract
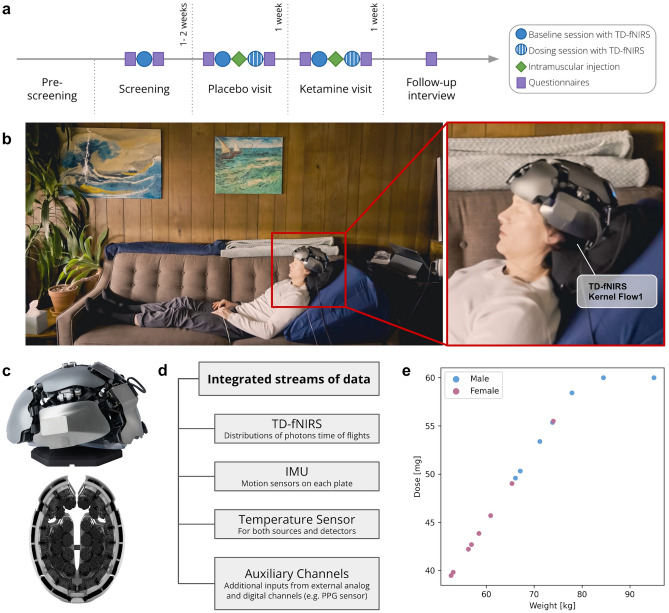
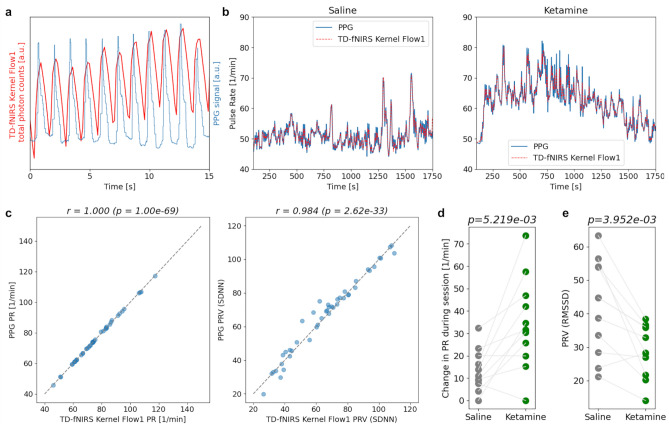
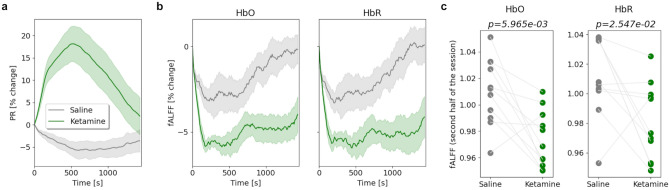
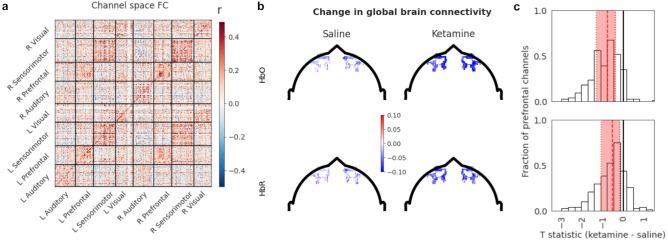
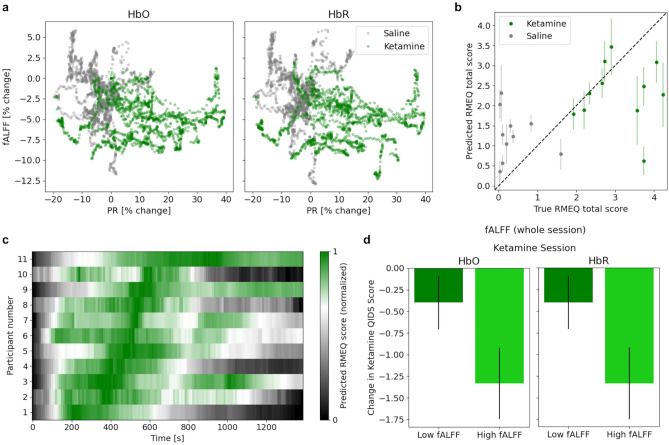
Quantifying neural activity in natural conditions (i.e. conditions comparable to the standard clinical patient experience) during the administration of psychedelics may further our scientific understanding of the effects and mechanisms of action. This data may facilitate the discovery of novel biomarkers enabling more personalized treatments and improved patient outcomes. In this single-blind, placebo-controlled study with a non-randomized design, we use time-domain functional near-infrared spectroscopy (TD-fNIRS) to measure acute brain dynamics after intramuscular subanesthetic ketamine (0.75 mg/kg) and placebo (saline) administration in healthy participants (n = 15, 8 females, 7 males, age 32.4 ± 7.5 years) in a clinical setting. We found that the ketamine administration caused an altered state of consciousness and changes in systemic physiology (e.g. increase in pulse rate and electrodermal activity). Furthermore, ketamine led to a brain-wide reduction in the fractional amplitude of low frequency fluctuations, and a decrease in the global brain connectivity of the prefrontal region. Lastly, we provide preliminary evidence that a combination of neural and physiological metrics may serve as predictors of subjective mystical experiences and reductions in depressive symptomatology. Overall, our study demonstrated the successful application of fNIRS neuroimaging to study the physiological effects of the psychoactive substance ketamine in humans, and can be regarded as an important step toward larger scale clinical fNIRS studies that can quantify the impact of psychedelics on the brain in standard clinical settings.
© 2023. The Author(s).
Conflict of interest statement
Authors AC, JD, RMF, FF, AG, WCH, SJ, JKH, ZMA, NM, KLP, JP, WCR, MS and MT were employed by Kernel during this study. FS provided scientific consulting for Kernel. The funder, Cybin, contributed to the conceptualization of this study and approved the final manuscript for submission.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
