

Innovative suture technique for robotic hepaticojejunostomy: double-layer interrupted sutures
- PMID: 37468703
- PMCID: PMC10356881
- DOI: 10.1007/s00423-023-03020-1
Innovative suture technique for robotic hepaticojejunostomy: double-layer interrupted sutures
Abstract
Purpose: Biliary reconstruction remains a technically demanding and complicated procedure in minimally invasive hepatopancreatobiliary surgeries. No optimal hepaticojejunostomy (HJ) technique has been demonstrated to be superior for preventing biliary complications. This study aimed to investigate the feasibility of our unique technique of posterior double-layer interrupted sutures in robotic HJ.
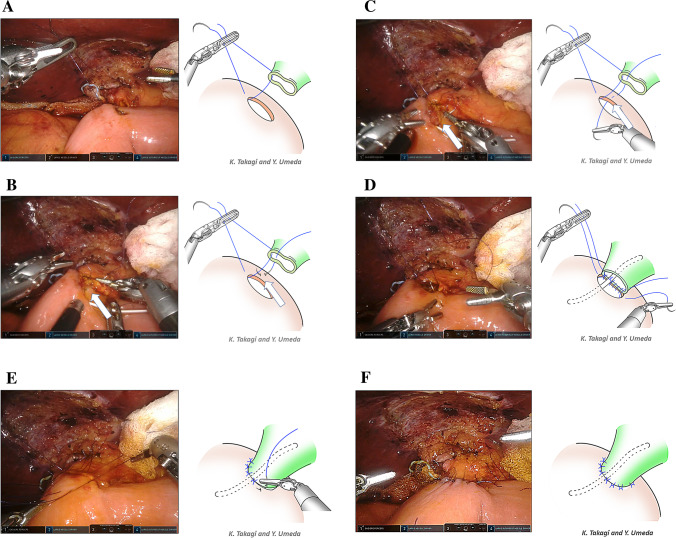
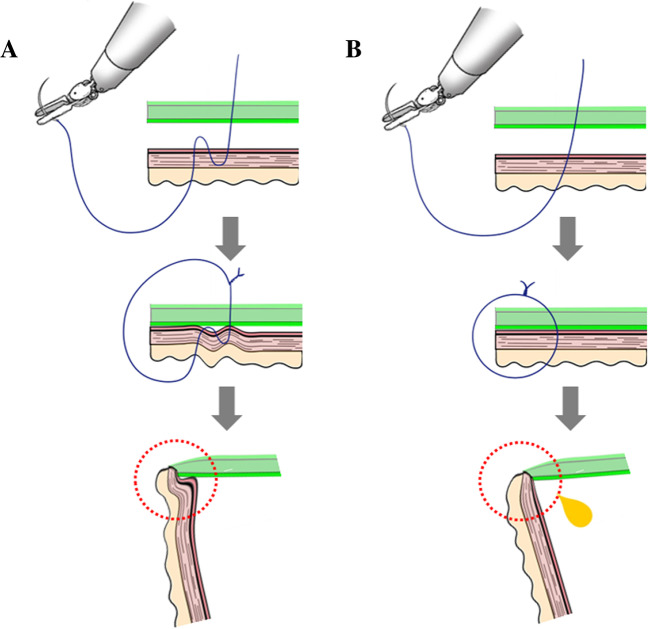
Methods: We performed a retrospective analysis of a prospectively collected database. Forty-two patients who underwent robotic pancreatoduodenectomy using this technique between September 2020 and November 2022 at our center were reviewed. In the posterior double-layer interrupted technique, sutures were placed to bite the bile duct, posterior seromuscular layer of the jejunum, and full thickness of the jejunum.
Results: The median operative time was 410 (interquartile range [IQR], 388-478) min, and the median HJ time was 30 (IQR, 28-39) min. The median bile duct diameter was 7 (IQR, 6-10) mm. Of the 42 patients, one patient (2.4%) had grade B bile leakage. During the median follow-up of 12.6 months, one patient (2.4%) with bile leakage developed anastomotic stenosis. Perioperative mortality was not observed. A surgical video showing the posterior double-layer interrupted sutures in the robotic HJ is included.
Conclusions: Posterior double-layer interrupted sutures in robotic HJ provided a simple and feasible method for biliary reconstruction with a low risk of biliary complications.
Keywords: Biliary complications; Hepaticojejunostomy; Pancreatoduodenectomy; Robotic surgery.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare no conflict of interest.
Figures
Similar articles
-
Biliary reconstruction with wide-interval interrupted suture to prevent biliary complications in pediatric living-donor liver transplantation.J Hepatobiliary Pancreat Sci. 2011 Jan;18(1):26-31. doi: 10.1007/s00534-010-0301-5. Epub 2010 Jul 3. J Hepatobiliary Pancreat Sci. 2011. PMID: 20602241
-
Incidence of anastomotic stricture after hepaticojejunostomy with continuous sutures in patients who underwent laparoscopic pancreaticoduodenectomy.Surg Today. 2021 Jul;51(7):1212-1219. doi: 10.1007/s00595-020-02223-z. Epub 2021 Jan 9. Surg Today. 2021. PMID: 33420821
-
Robotic Klatskin Type 3A Resection with Biliary Reconstruction: Description of Surgical Technique and Outcomes of Initial Series.Ann Surg Oncol. 2023 Dec;30(13):8559-8560. doi: 10.1245/s10434-023-14256-y. Epub 2023 Sep 8. Ann Surg Oncol. 2023. PMID: 37684368
-
Meta-analysis of interrupted versus continuous suturing for Roux-en-Y hepaticojejunostomy and duct-to-duct choledochocholedochostomy.Langenbecks Arch Surg. 2022 Aug;407(5):1817-1829. doi: 10.1007/s00423-022-02548-y. Epub 2022 May 13. Langenbecks Arch Surg. 2022. PMID: 35552518
-
Techniques of biliary reconstruction following bile duct resection (with video).J Hepatobiliary Pancreat Sci. 2012 May;19(3):203-9. doi: 10.1007/s00534-011-0475-5. J Hepatobiliary Pancreat Sci. 2012. PMID: 22081253 Free PMC article. Review.
Cited by
-
Impact of internal stent placement on late biliary complications after robot-assisted pancreaticoduodenectomy.Surg Endosc. 2025 Jul 18. doi: 10.1007/s00464-025-11805-2. Online ahead of print. Surg Endosc. 2025. PMID: 40681649
-
The state of robotic vs. open pancreatoduodenectomy.Gland Surg. 2024 Aug 31;13(8):1344-1348. doi: 10.21037/gs-24-182. Epub 2024 Aug 20. Gland Surg. 2024. PMID: 39282045 Free PMC article. No abstract available.
-
Treatment of hemolymphangioma by robotic surgery: A case report.World J Gastrointest Surg. 2024 Feb 27;16(2):596-600. doi: 10.4240/wjgs.v16.i2.596. World J Gastrointest Surg. 2024. PMID: 38463376 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
