

Cost-effectiveness of prehabilitation prior to elective surgery: a systematic review of economic evaluations
- PMID: 37468923
- PMCID: PMC10354976
- DOI: 10.1186/s12916-023-02977-6
Cost-effectiveness of prehabilitation prior to elective surgery: a systematic review of economic evaluations
Abstract
Background: Prehabilitation aims at enhancing patients' functional capacity and overall health status to enable them to withstand a forthcoming stressor like surgery. Our aim was to synthesise the evidence on the cost-effectiveness of prehabilitation for patients awaiting elective surgery compared with usual preoperative care.
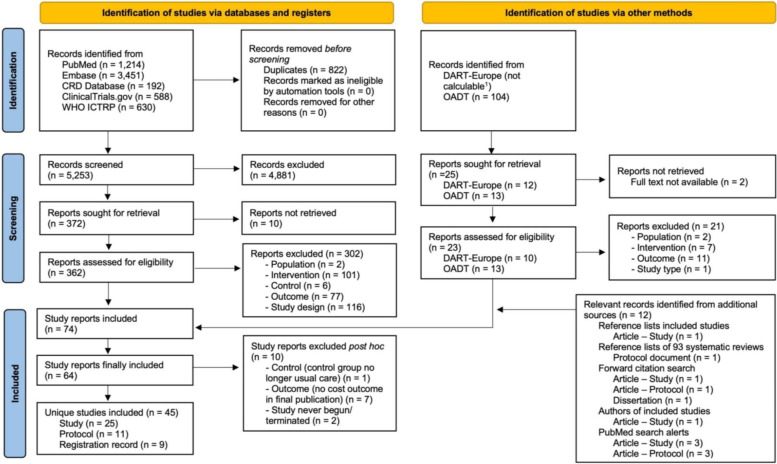
Methods: We searched PubMed, Embase, the CRD database, ClinicalTrials.gov, the WHO ICTRP and the dissertation databases OADT and DART. Studies comparing prehabilitation for patients with elective surgery to usual preoperative care were included if they reported cost outcomes. All types of economic evaluations (EEs) were included. The primary outcome of the review was cost-effectiveness based on cost-utility analyses (CUAs). The risk of bias of trial-based EEs was assessed with the Cochrane risk of bias 2 tool and the ROBINS-I tool and the credibility of model-based EEs with the ISPOR checklist. Methodological quality of full EEs was assessed using the CHEC checklist. The EEs' results were synthesised narratively using vote counting based on direction of effect.
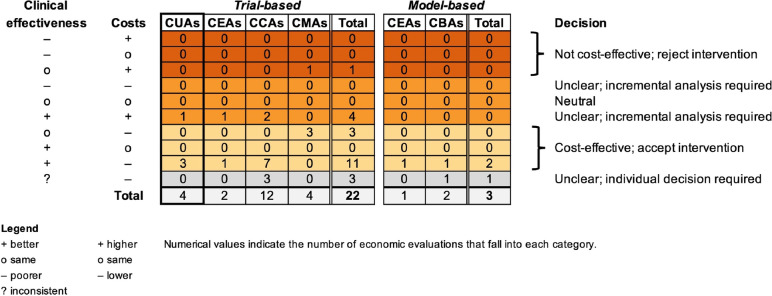
Results: We included 45 unique studies: 25 completed EEs and 20 ongoing studies. Of the completed EEs, 22 were trial-based and three model-based, corresponding to four CUAs, three cost-effectiveness analyses, two cost-benefit analyses, 12 cost-consequence analyses and four cost-minimization analyses. Three of the four trial-based CUAs (75%) found prehabilitation cost-effective, i.e. more effective and/or less costly than usual care. Overall, 16/25 (64.0%) EEs found prehabilitation cost-effective. When excluding studies of insufficient credibility/critical risk of bias, this number reduced to 14/23 (60.9%). In 8/25 (32.0%), cost-effectiveness was unclear, e.g. because prehabilitation was more effective and more costly, and in one EE prehabilitation was not cost-effective.
Conclusions: We found some evidence that prehabilitation for patients awaiting elective surgery is cost-effective compared to usual preoperative care. However, we suspect a relevant risk of publication bias, and most EEs were of high risk of bias and/or low methodological quality. Furthermore, there was relevant heterogeneity depending on the population, intervention and methods. Future EEs should be performed over a longer time horizon and apply a more comprehensive perspective.
Trial registration: PROSPERO CRD42020182813.
Keywords: Cost-effectiveness; Evidence synthesis; Health economics; Prehabilitation; Systematic review.
© 2023. The Author(s).
Conflict of interest statement
TR, HE, JS, JK and WQ are involved in one of the included ongoing economic evaluations [59]. TM declares to have no competing interests.
Figures
Similar articles
-
Immediate sequential bilateral surgery versus delayed sequential bilateral surgery for cataracts.Cochrane Database Syst Rev. 2022 Apr 25;4(4):CD013270. doi: 10.1002/14651858.CD013270.pub2. Cochrane Database Syst Rev. 2022. PMID: 35467755 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
Cited by
-
Prehabilitation in Major Surgery: An Evaluation of Cost Savings in a Tertiary Hospital.J Clin Med. 2025 Apr 3;14(7):2460. doi: 10.3390/jcm14072460. J Clin Med. 2025. PMID: 40217909 Free PMC article.
-
Factors predicting outcomes from chronic pain management interventions.BMJ Med. 2025 Jul 7;4(1):e001143. doi: 10.1136/bmjmed-2024-001143. eCollection 2025. BMJ Med. 2025. PMID: 40735511 Free PMC article. Review.
-
Cost-effectiveness of prehabilitation of elderly frail or pre-frail patients prior to elective surgery (PRAEP-GO) versus usual care - Protocol for a health economic evaluation alongside a randomized controlled trial.BMC Geriatr. 2024 Mar 6;24(1):231. doi: 10.1186/s12877-024-04833-5. BMC Geriatr. 2024. PMID: 38448804 Free PMC article.
-
Can We Empower Patients for Joint Surgery? Assessing the Impact of a Telemedicine Coaching Intervention.Arthroplast Today. 2025 May 6;33:101701. doi: 10.1016/j.artd.2025.101701. eCollection 2025 Jun. Arthroplast Today. 2025. PMID: 40635730 Free PMC article.
-
Effects of Prehabilitation With Advanced Technologies in Patients With Musculoskeletal Diseases Waiting for Surgery: Systematic Review and Meta-Analysis.J Med Internet Res. 2024 Dec 12;26:e52943. doi: 10.2196/52943. J Med Internet Res. 2024. PMID: 39666971 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
