

Wedge resection versus segment IVb and V resection of the liver for T2 gallbladder cancer: a systematic review and meta-analysis
- PMID: 37469411
- PMCID: PMC10352769
- DOI: 10.3389/fonc.2023.1186378
Wedge resection versus segment IVb and V resection of the liver for T2 gallbladder cancer: a systematic review and meta-analysis
Abstract
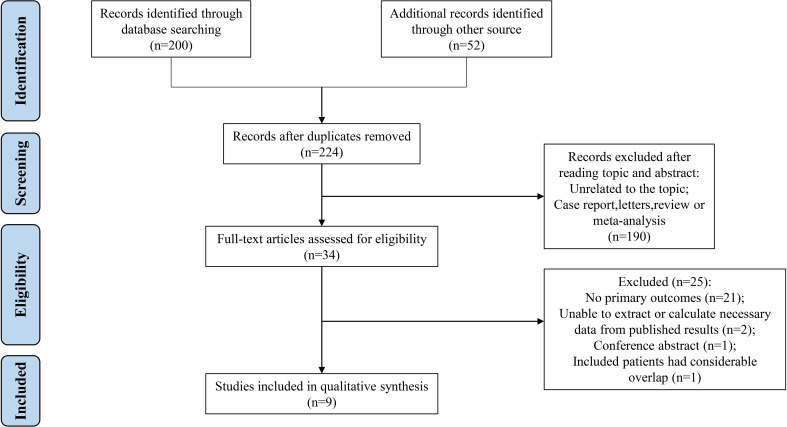
Objectives: Although guidelines recommend extended cholecystectomy for T2 gallbladder cancer (GBC), the optimal hepatectomy strategy remains controversial. The study aims to compare the prognosis of T2 GBC patients who underwent wedge resection (WR) versus segment IVb and V resection (SR) of the liver.
Methods: A specific search of online databases was performed from May 2001 to February 2023. The postoperative efficacy outcomes were synthesized and meta-analyses were conducted.
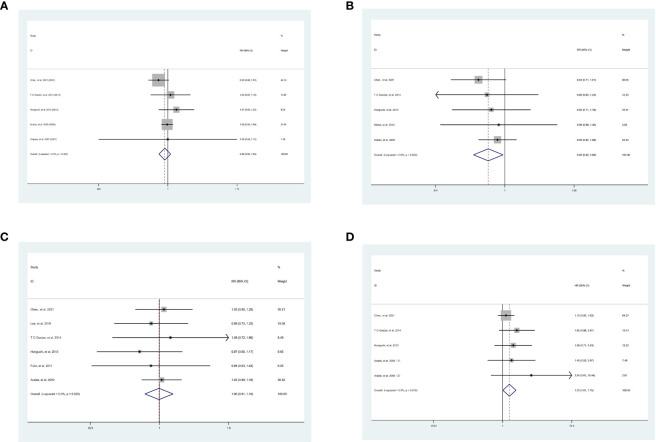
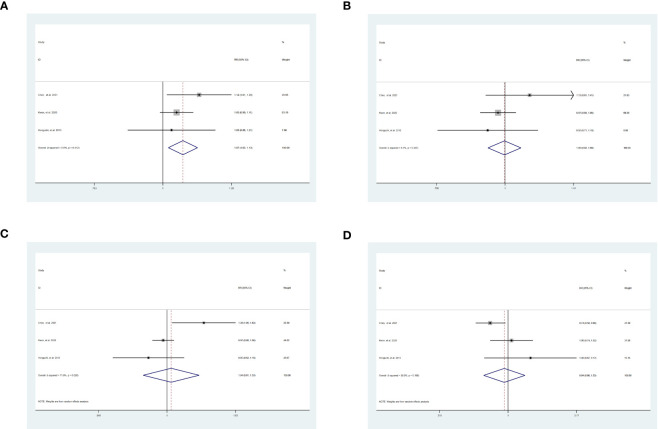
Results: A total of 9 studies involving 2,086 (SR = 627, WR = 1,459) patients were included in the study. The primary outcomes included disease-free survival (DFS) and overall survival (OS). For DFS, the 1-year DFS was statistically higher in patients undergoing SR than WR [risk ratio (RR) = 1.07, 95% confidence interval (CI) = 1.02-1.13, P = 0.007]. The 3-year DFS (P = 0.95), 5-year DFS (P = 0.77), and hazard ratio (HR) of DFS (P = 0.72) were similar between the two groups. However, the 3-year OS was significantly lower in patients who underwent SR than WR [RR = 0.90, 95% CI = 0.82-0.99, P = 0.03]. Moreover, SR had a higher hazard HR of OS [HR = 1.33, 95% CI = 1.01-1.75, P = 0.04]. No significant difference was found in 1-year (P = 0.32) and 5-year (P = 0.9) OS. For secondary outcomes, patients who received SR tended to develop postoperative complications (POC) [RR = 1.90, 95% CI = 1.00-3.60, P = 0.05]. In addition, no significant differences in intrahepatic recurrence (P = 0.12) were observed.
Conclusions: In conclusion, SR can improve the prognosis of T2 GBC patients in DFS. In contrast to WR, the high HR and complications associated with SR cannot be neglected. Therefore, surgeons should evaluate the condition of the patients and take their surgical skills into account when selecting SR.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier, CRD42022362974.
Keywords: gallbladder cancer; meta-analysis; prognosis; segment IVb/V resection; wedge resection.
Copyright © 2023 Chen, Yu, Cao, Lin, Hu, Zhang, Shen, Feng, Topatana, Chen and Fang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Surgical and Oncological Outcomes of Wedge Resection Versus Segment 4b + 5 Resection for T2 and T3 Gallbladder Cancer: a Meta-Analysis.J Gastrointest Surg. 2023 Sep;27(9):1954-1962. doi: 10.1007/s11605-023-05698-6. Epub 2023 May 23. J Gastrointest Surg. 2023. PMID: 37221386 Review.
-
Hepatectomy strategy for T2 gallbladder cancer between segment IVb and V resection and wedge resection: A propensity score-matched study.Surgery. 2021 Jun;169(6):1304-1311. doi: 10.1016/j.surg.2020.12.039. Epub 2021 Feb 5. Surgery. 2021. PMID: 33551070
-
Managing the incidentally detected gallbladder cancer: algorithms and controversies.Int J Surg. 2014;12 Suppl 2:S108-S119. doi: 10.1016/j.ijsu.2014.08.367. Epub 2014 Aug 23. Int J Surg. 2014. PMID: 25182380
-
Long-Term Oncologic Outcomes for T2 Gallbladder Cancer According to the Type of Surgery Performed and the Optimal Timing for Sequential Extended Cholecystectomy.J Gastrointest Surg. 2022 Aug;26(8):1705-1712. doi: 10.1007/s11605-022-05368-z. Epub 2022 May 31. J Gastrointest Surg. 2022. PMID: 35641810
-
Effect of simple vs. extended cholecystectomy on prognosis of T1b gallbladder cancer: a systematic review and meta-analysis.Front Surg. 2025 May 26;12:1477301. doi: 10.3389/fsurg.2025.1477301. eCollection 2025. Front Surg. 2025. PMID: 40491426 Free PMC article.
Cited by
-
New trends in diagnosis and management of gallbladder carcinoma.World J Gastrointest Oncol. 2024 Jan 15;16(1):13-29. doi: 10.4251/wjgo.v16.i1.13. World J Gastrointest Oncol. 2024. PMID: 38292841 Free PMC article. Review.
-
Long-term survival of stage 4 gallbladder cancer after extended radical surgery plus limited chemotherapy: a case report.J Surg Case Rep. 2025 Jan 20;2025(1):rjaf010. doi: 10.1093/jscr/rjaf010. eCollection 2025 Jan. J Surg Case Rep. 2025. PMID: 39834473 Free PMC article.
References
-
- Horiguchi A, Miyakawa S, Ishihara S, Miyazaki M, Ohtsuka M, Shimizu H, et al. . Gallbladder bed resection or hepatectomy of segments 4a and 5 for pT2 gallbladder carcinoma: analysis of Japanese registration cases by the study group for biliary surgery of the Japanese society of hepato-Biliary-Pancreatic surgery. J Hepatobiliary Pancreat Sci (2013) 20:518–24. doi: 10.1007/s00534-012-0584-9 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials