

Age, blood tests and comorbidities and AIMS65 risk scores outperform Glasgow-Blatchford and pre-endoscopic Rockall score in patients with upper gastrointestinal bleeding
- PMID: 37469720
- PMCID: PMC10353516
- DOI: 10.12998/wjcc.v11.i19.4513
Age, blood tests and comorbidities and AIMS65 risk scores outperform Glasgow-Blatchford and pre-endoscopic Rockall score in patients with upper gastrointestinal bleeding
Abstract
Background: Upper gastrointestinal (GI) bleeding is a life-threatening condition with high mortality rates.
Aim: To compare the performance of pre-endoscopic risk scores in predicting the following primary outcomes: In-hospital mortality, intervention (endoscopic or surgical) and length of admission (≥ 7 d).
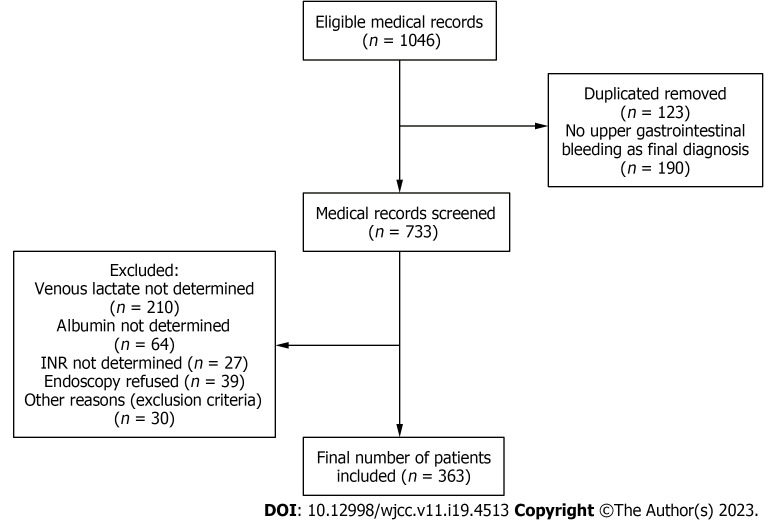
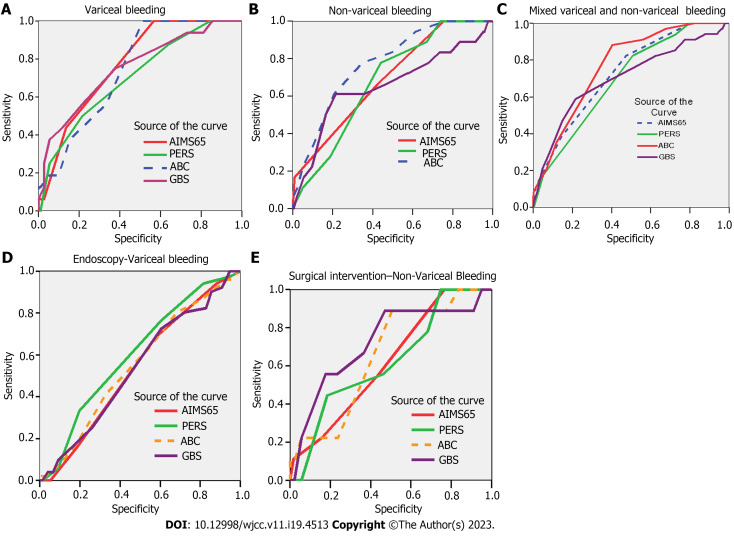
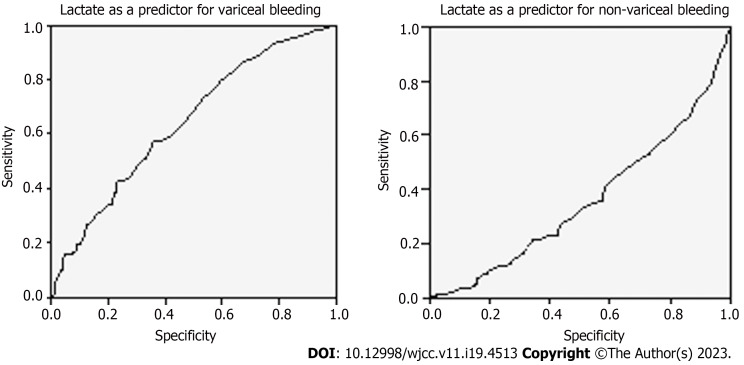
Methods: We performed a retrospective analysis of 363 patients presenting with upper GI bleeding from December 2020 to January 2021. We calculated and compared the area under the receiver operating characteristics curves (AUROCs) of Glasgow-Blatchford score (GBS), pre-endoscopic Rockall score (PERS), albumin, international normalized ratio, altered mental status, systolic blood pressure, age older than 65 (AIMS65) and age, blood tests and comorbidities (ABC), including their optimal cut-off in variceal and non-variceal upper GI bleeding cohorts. We subsequently analyzed through a logistic binary regression model, if addition of lactate increased the score performance.
Results: All scores had discriminative ability in predicting in-hospital mortality irrespective of study group. AIMS65 score had the best performance in the variceal bleeding group (AUROC = 0.772; P < 0.001), and ABC score (AUROC = 0.775; P < 0.001) in the non-variceal bleeding group. However, ABC score, at a cut-off value of 5.5, was the best predictor (AUROC = 0.770, P = 0.001) of in-hospital mortality in both populations. PERS score was a good predictor for endoscopic treatment (AUC = 0.604; P = 0.046) in the variceal population, while GBS score, (AUROC = 0.722; P = 0.024), outperformed the other scores in predicting surgical intervention. Addition of lactate to AIMS65 score, increases by 5-fold the probability of in-hospital mortality (P < 0.05) and by 12-fold if added to GBS score (P < 0.003). No score proved to be a good predictor for length of admission.
Conclusion: ABC score is the most accurate in predicting in-hospital mortality in both mixed and non-variceal bleeding population. PERS and GBS should be used to determine need for endoscopic and surgical intervention, respectively. Lactate can be used as an additional tool to risk scores for predicting in-hospital mortality.
Keywords: Age older than 65; Age, blood tests and comorbidities; Gastrointestinal bleeding; Glasgow-Blatchford; Pre-endoscopic Rockall; Risk score.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflict of interest.
Figures
References
-
- Stanley AJ, Ashley D, Dalton HR, Mowat C, Gaya DR, Thompson E, Warshow U, Groome M, Cahill A, Benson G, Blatchford O, Murray W. Outpatient management of patients with low-risk upper-gastrointestinal haemorrhage: multicentre validation and prospective evaluation. Lancet. 2009;373:42–47. - PubMed
-
- Gralnek IM, Stanley AJ, Morris AJ, Camus M, Lau J, Lanas A, Laursen SB, Radaelli F, Papanikolaou IS, Cúrdia Gonçalves T, Dinis-Ribeiro M, Awadie H, Braun G, de Groot N, Udd M, Sanchez-Yague A, Neeman Z, van Hooft JE. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline-Update 2021. Endoscopy. 2021;53:300–332. - PubMed
-
- Stanley AJ, Dalton HR, Blatchford O, Ashley D, Mowat C, Cahill A, Gaya DR, Thompson E, Warshow U, Hare N, Groome M, Benson G, Murray W. Multicentre comparison of the Glasgow Blatchford and Rockall Scores in the prediction of clinical end-points after upper gastrointestinal haemorrhage. Aliment Pharmacol Ther. 2011;34:470–475. - PubMed
LinkOut - more resources
Full Text Sources
