

Derivation of an Outcome-Driven Threshold for Aortic Pulse Wave Velocity: An Individual-Participant Meta-Analysis
- PMID: 37470187
- PMCID: PMC10424824
- DOI: 10.1161/HYPERTENSIONAHA.123.21318
Derivation of an Outcome-Driven Threshold for Aortic Pulse Wave Velocity: An Individual-Participant Meta-Analysis
Abstract
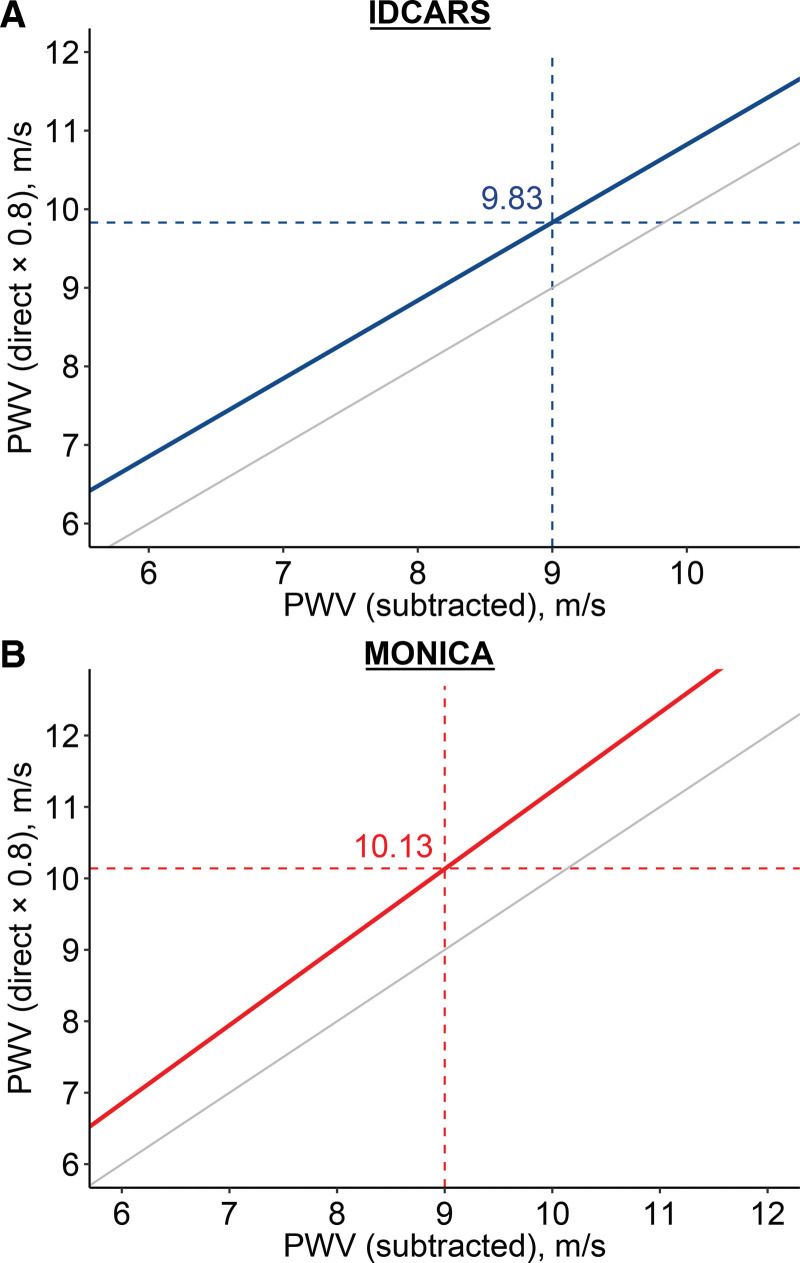
Background: Aortic pulse wave velocity (PWV) predicts cardiovascular events (CVEs) and total mortality (TM), but previous studies proposing actionable PWV thresholds have limited generalizability. This individual-participant meta-analysis is aimed at defining, testing calibration, and validating an outcome-driven threshold for PWV, using 2 populations studies, respectively, for derivation IDCARS (International Database of Central Arterial Properties for Risk Stratification) and replication MONICA (Monitoring of Trends and Determinants in Cardiovascular Disease Health Survey - Copenhagen).
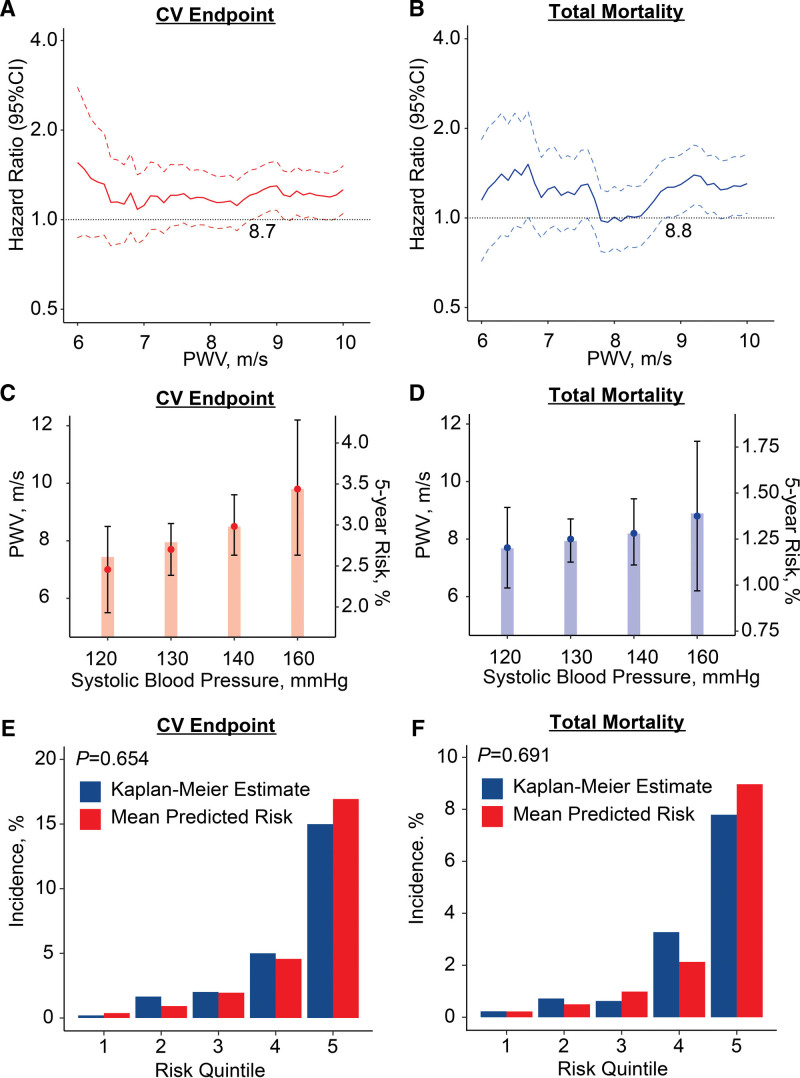
Methods: A risk-carrying PWV threshold for CVE and TM was defined by multivariable Cox regression, using stepwise increasing PWV thresholds and by determining the threshold yielding a 5-year risk equivalent with systolic blood pressure of 140 mm Hg. The predictive performance of the PWV threshold was assessed by computing the integrated discrimination improvement and the net reclassification improvement.
Results: In well-calibrated models in IDCARS, the risk-carrying PWV thresholds converged at 9 m/s (10 m/s considering the anatomic pulse wave travel distance). With full adjustments applied, the threshold predicted CVE (hazard ratio [CI]: 1.68 [1.15-2.45]) and TM (1.61 [1.01-2.55]) in IDCARS and in MONICA (1.40 [1.09-1.79] and 1.55 [1.23-1.95]). In IDCARS and MONICA, the predictive accuracy of the threshold for both end points was ≈0.75. Integrated discrimination improvement was significant for TM in IDCARS and for both TM and CVE in MONICA, whereas net reclassification improvement was not for any outcome.
Conclusions: PWV integrates multiple risk factors into a single variable and might replace a large panel of traditional risk factors. Exceeding the outcome-driven PWV threshold should motivate clinicians to stringent management of risk factors, in particular hypertension, which over a person's lifetime causes stiffening of the elastic arteries as waypoint to CVE and death.
Keywords: cardiovascular diseases; diabetes mellitus; hypertension; metabolic syndrome; pulse wave analysis.
Conflict of interest statement
Figures
References
-
- Van Bortel LM, Laurent S, Boutouyrie P, Chowienczyk P, Cruickshank JK, De Backer T, Filipovsky J, Huybrechts S, Mattace-Raso FU, Protogerou AD, et al. ; Artery Society. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J Hypertens. 2012;30:445–448. doi: 10.1097/HJH.0b013e32834fa8b0 - PubMed
-
- Mancia G, De BG, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, et al. . 2007 ESH-ESC practice Guidelines for the management of arterial hypertension: ESH-ESC task force on the management of arterial hypertension. J Hypertens. 2007;25:1751–1762. doi: 10.1097/HJH.0b013e3282f0580f - PubMed
-
- Joint Committee for Guideline Revision. 2018 Chinese guidelines for prevention and treatment of hypertension — a report of the Revision Committee of Chinese Guidelines for Prevention and Treatment of Hypertension. J Geriatr Cardiol. 2022;16:182–241. doi: 10.11909/j.issn.1671-5411.2019.03.014 - PMC - PubMed
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, et al. ; ESC Scientific Document Group. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–3104. doi: 10.1093/eurheartj/ehy339 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
