

Balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: a clinical consensus statement of the ESC working group on pulmonary circulation and right ventricular function
- PMID: 37470202
- PMCID: PMC10393078
- DOI: 10.1093/eurheartj/ehad413
Balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: a clinical consensus statement of the ESC working group on pulmonary circulation and right ventricular function
Abstract
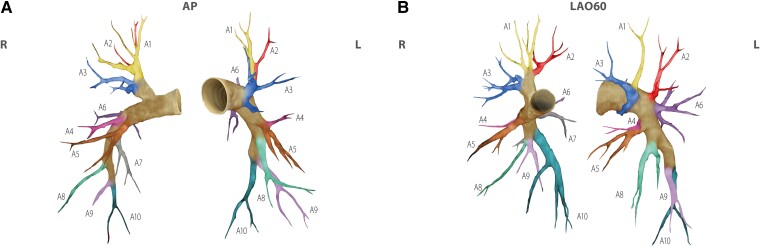
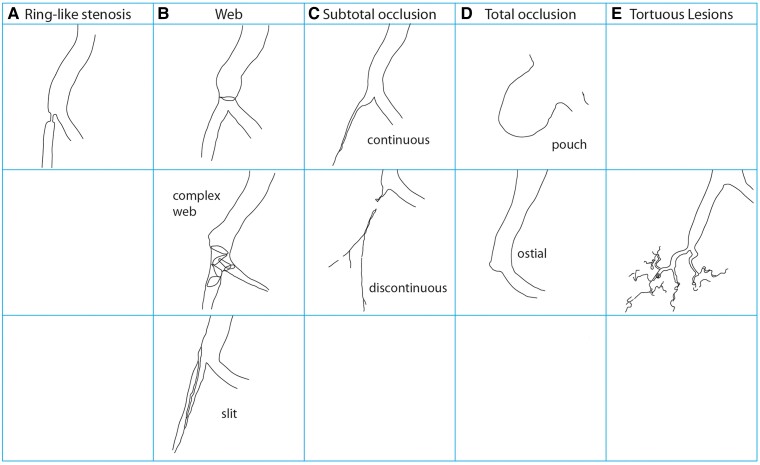
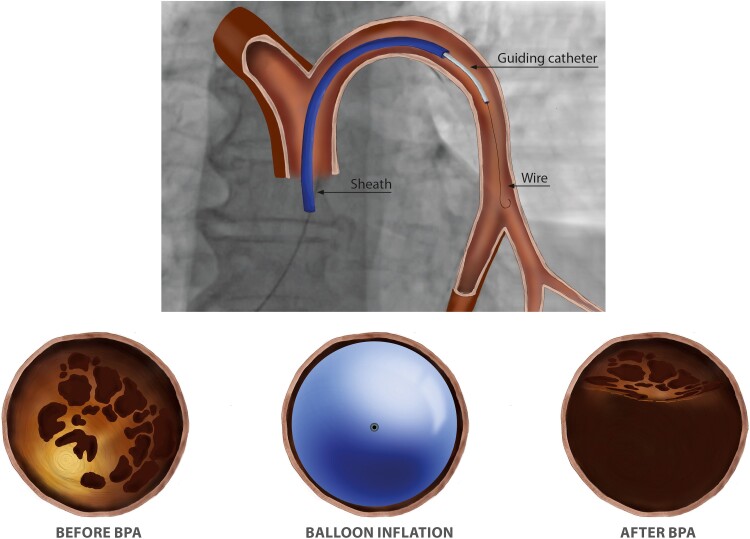
The current treatment algorithm for chronic thromboembolic pulmonary hypertension (CTEPH) as depicted in the 2022 European Society of Cardiology (ESC)/European Respiratory Society (ERS) guidelines on the diagnosis and treatment of pulmonary hypertension (PH) includes a multimodal approach of combinations of pulmonary endarterectomy (PEA), balloon pulmonary angioplasty (BPA) and medical therapies to target major vessel pulmonary vascular lesions, and microvasculopathy. Today, BPA of >1700 patients has been reported in the literature from centers in Asia, the US, and also Europe; many more patients have been treated outside literature reports. As BPA becomes part of routine care of patients with CTEPH, benchmarks for safe and effective care delivery become increasingly important. In light of this development, the ESC Working Group on Pulmonary Circulation and Right Ventricular Function has decided to publish a document that helps standardize BPA to meet the need of uniformity in patient selection, procedural planning, technical approach, materials and devices, treatment goals, complications including their management, and patient follow-up, thus complementing the guidelines. Delphi methodology was utilized for statements that were not evidence based. First, an anatomical nomenclature and a description of vascular lesions are provided. Second, treatment goals and definitions of complete BPA are outlined. Third, definitions of complications are presented which may be the basis for a standardized reporting in studies involving BPA. The document is intended to serve as a companion to the official ESC/ERS guidelines.
Keywords: Balloon pulmonary angioplasty; Chronic thromboembolic pulmonary disease; Chronic thromboembolic pulmonary hypertension.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
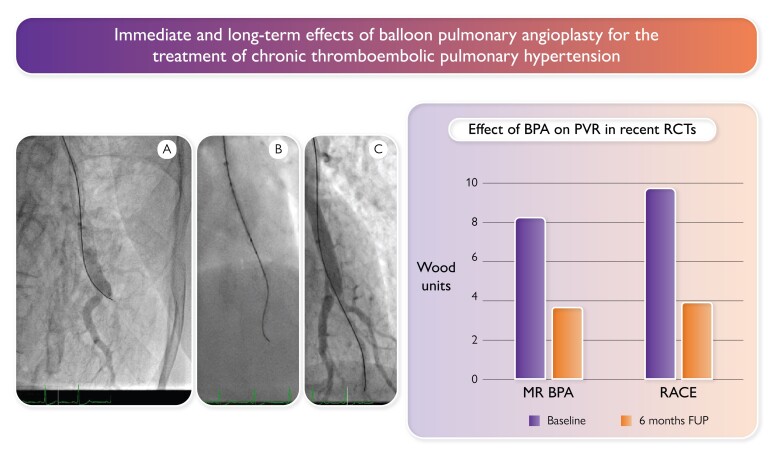
- Kawakami T, Matsubara H, Shinke T, Abe K, Kohsaka S, Hosokawa K, et al. Balloon pulmonary angioplasty versus riociguat in inoperable chronic thromboembolic pulmonary hypertension (MR BPA): an open-label, randomised controlled trial. Lancet Respir Med 2022;10:949–960. 10.1016/S2213-2600(22)00171-0 - DOI - PubMed
-
- Jaïs X, Brenot P, Bouvaist H, Jevnikar M, Canuet M, Chabanne C, et al. Balloon pulmonary angioplasty versus riociguat for the treatment of inoperable chronic thromboembolic pulmonary hypertension (RACE): a multicentre, phase 3, open-label, randomised controlled trial and ancillary follow-up study. Lancet Respir Med 2022;10:961–971. 10.1016/S2213-2600(22)00214-4 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
