

Manual vs. automatic assessment of the QT-interval and corrected QT
- PMID: 37470430
- PMCID: PMC10469369
- DOI: 10.1093/europace/euad213
Manual vs. automatic assessment of the QT-interval and corrected QT
Abstract
Aims: Sudden cardiac death (SCD) is challenging to predict. Electrocardiogram (ECG)-derived heart rate-corrected QT-interval (QTc) is used for SCD-risk assessment. QTc is preferably determined manually, but vendor-provided automatic results from ECG recorders are convenient. Agreement between manual and automatic assessments is unclear for populations with aberrant QTc. We aimed to systematically assess pairwise agreement of automatic and manual QT-intervals and QTc.
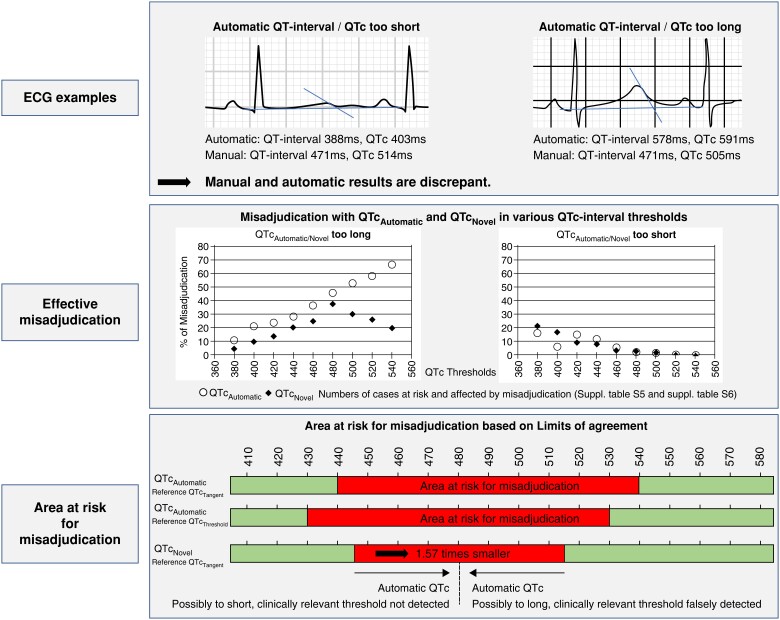
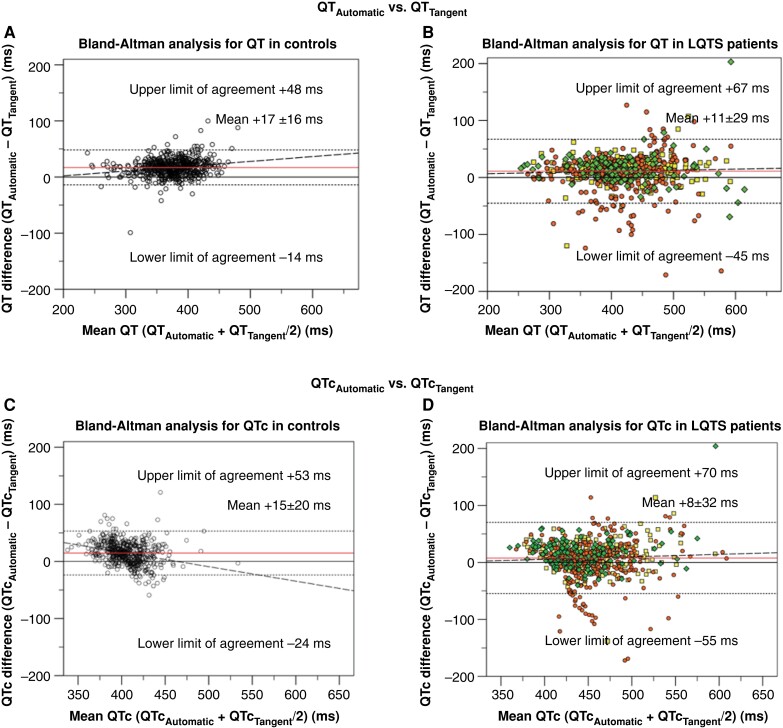
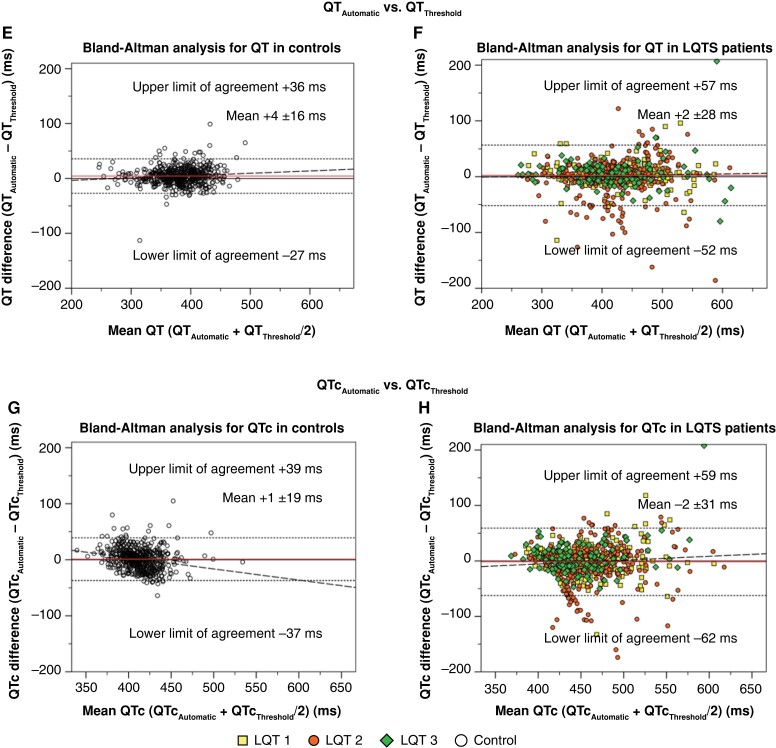
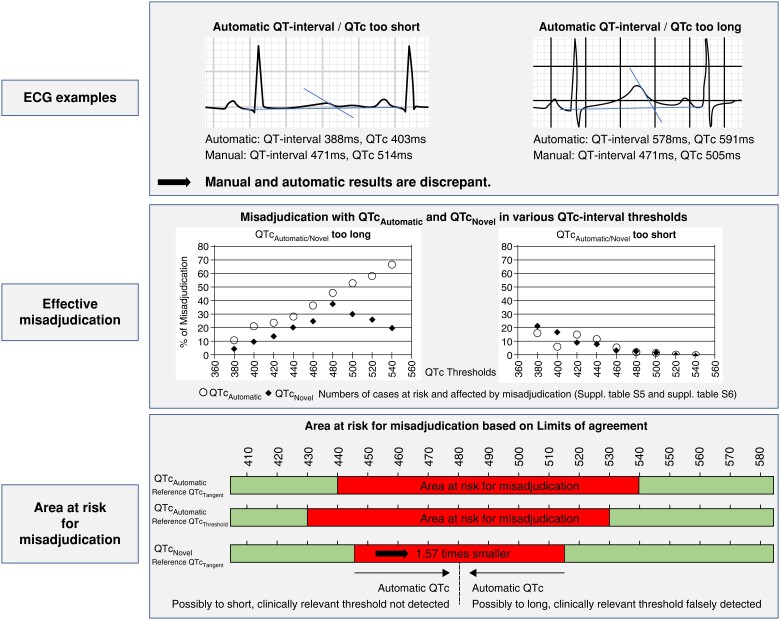
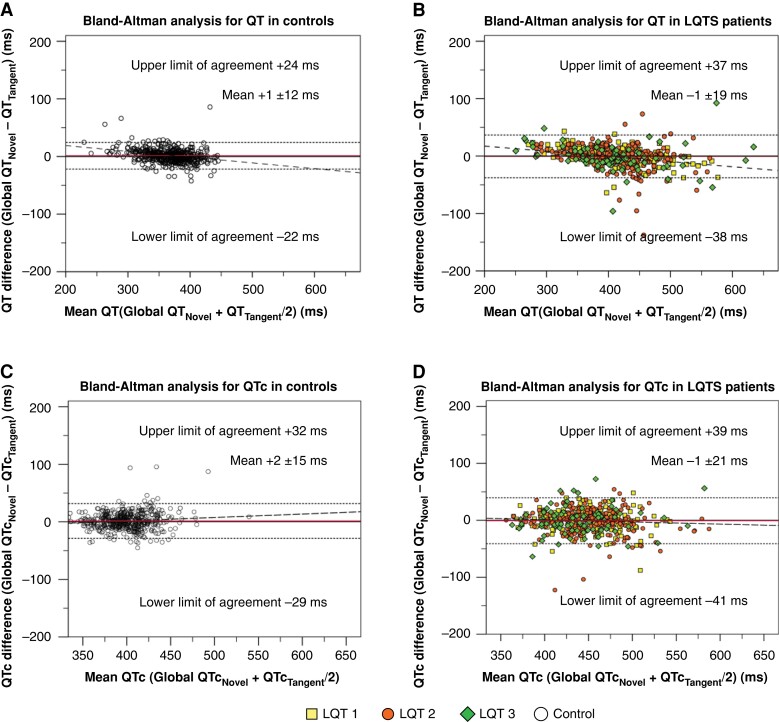
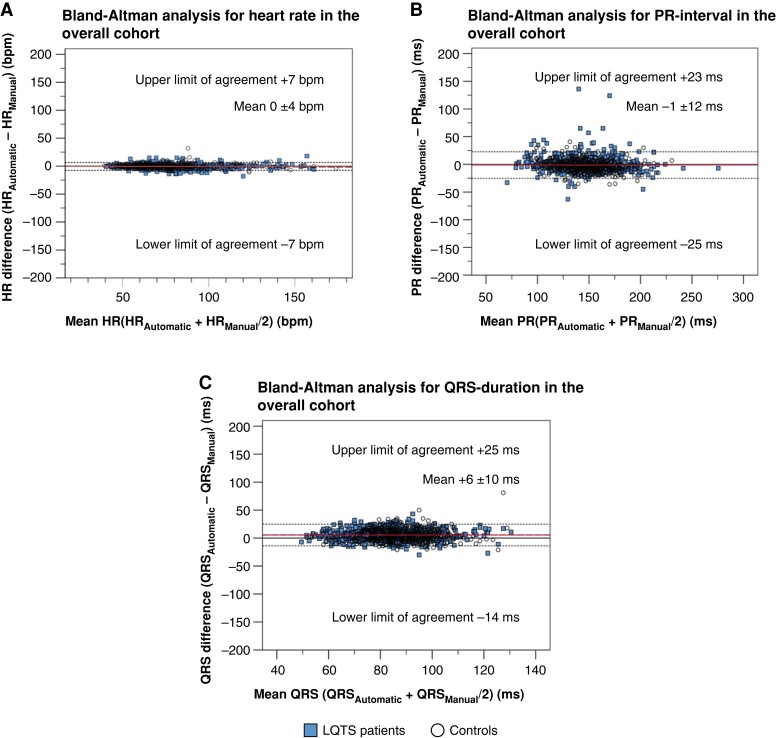
Methods and results: A multi-centre cohort enriching aberrant QTc comprised ECGs of healthy controls and long-QT syndrome (LQTS) patients. Manual QT-intervals and QTc were determined by the tangent and threshold methods and compared to automatically generated, vendor-provided values. We assessed agreement globally by intra-class correlation coefficients and pairwise by Bland-Altman analyses and 95% limits of agreement (LoA). Further, manual results were compared to a novel automatic QT-interval algorithm. ECGs of 1263 participants (720 LQTS patients; 543 controls) were available [median age 34 (inter-quartile range 35) years, 55% women]. Comparing cohort means, automatic and manual QT-intervals and QTc were similar. However, pairwise Bland-Altman-based agreement was highly discrepant. For QT-interval, LoAs spanned 95 (tangent) and 92 ms (threshold), respectively. For QTc, the spread was 108 and 105 ms, respectively. LQTS patients exhibited more pronounced differences. For automatic QTc results from 440-540 ms (tangent) and 430-530 ms (threshold), misassessment risk was highest. Novel automatic QT-interval algorithms may narrow this range.
Conclusion: Pairwise vendor-provided automatic and manual QT-interval and QTc results can be highly discrepant. Novel automatic algorithms may improve agreement. Within the above ranges, automatic QT-interval and QTc results require manual confirmation, particularly if T-wave morphology is challenging.
Keywords: Electrocardiogram; Long QT syndrome; Misassessment; QT-interval; QTc; Sudden cardiac death.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Bagnall RD, Weintraub RG, Ingles J, Duflou J, Yeates L, Lam Let al. . A prospective study of sudden cardiac death among children and young adults. N Engl J Med 2016;374:2441–52. - PubMed
-
- Eckart RE, Shry EA, Burke AP, McNear JA, Appel DA, Castillo-Rojas LMet al. . Sudden death in young adults: an autopsy-based series of a population undergoing active surveillance. J Am Coll Cardiol 2011;58:1254–61. - PubMed
-
- Priori SG, Aliot E, Blomstrom-Lundqvist C, Bossaert L, Breithardt G, Brugada Pet al. . Task force on sudden cardiac death of the European society of cardiology. Eur Heart J 2001;22:1374–450. - PubMed
-
- Myerburg RJ, Goldberger JJ. Sudden cardiac arrest risk assessment: population science and the individual risk mandate. JAMA Cardiol 2017;2:689–94. - PubMed
-
- Al-Khatib SM, Stevenson WG, Ackerman MJ, Bryant WJ, Callans DJ, Curtis ABet al. . 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society. Heart Rhythm 2018;15:e190–252. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
