

Chimeric Antigen Receptor T-Cell and Bispecific Antibody Therapy in Multiple Myeloma: Moving Into the Future
- PMID: 37471687
- PMCID: PMC10522112
- DOI: 10.1200/JCO.23.00512
Chimeric Antigen Receptor T-Cell and Bispecific Antibody Therapy in Multiple Myeloma: Moving Into the Future
Abstract
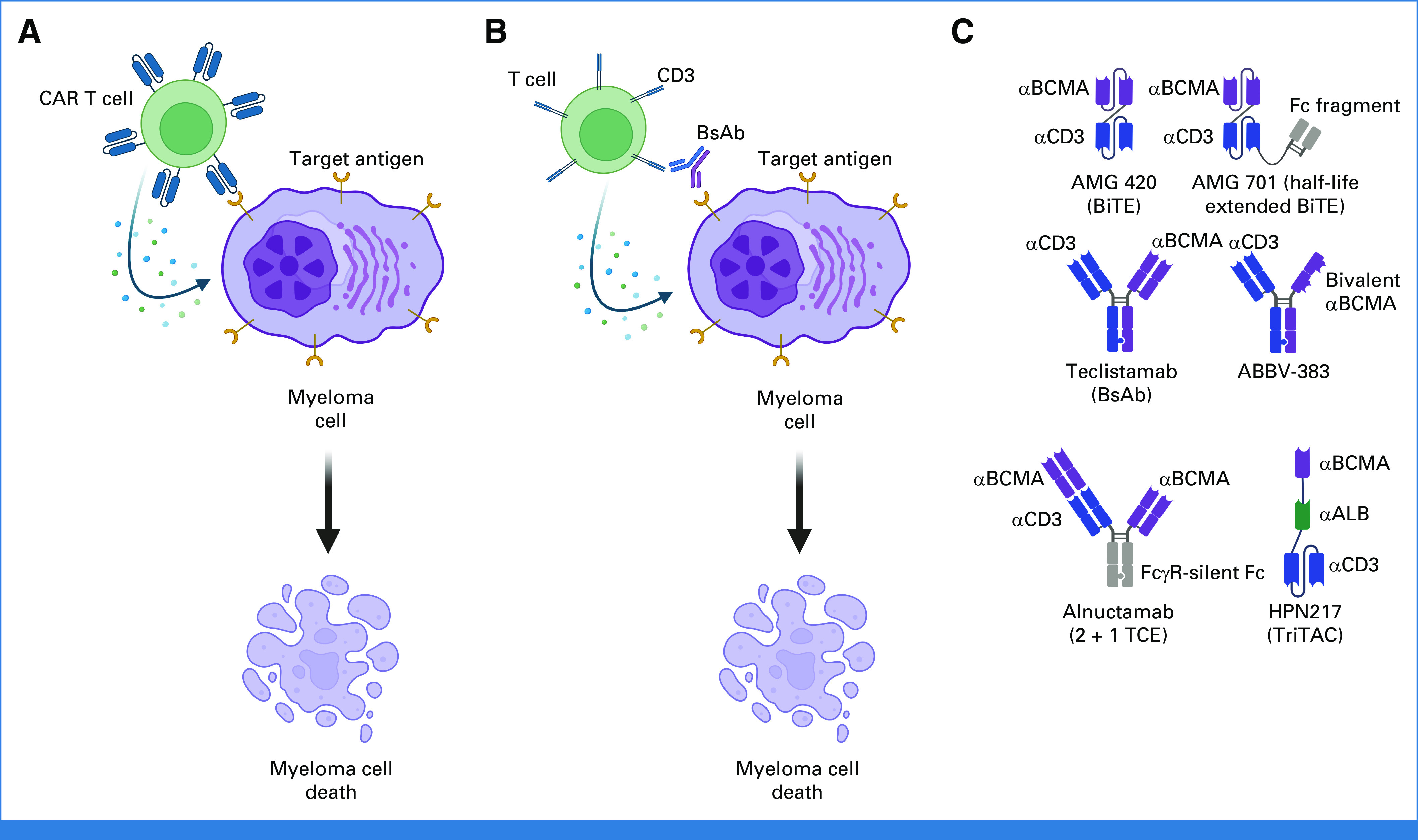
Historically, the outcomes for individuals with triple-class refractory and penta-drug refractory multiple myeloma (MM) have been poor because of a dearth of effective treatment options. However, the advent of chimeric antigen receptor (CAR) T-cell and T-cell redirecting bispecific antibody (BsAb) therapies has led to unprecedented response rates and durations of response in heavily relapsed/refractory (R/R) populations. Currently, two B-cell maturation antigen (BCMA)-directed CAR T-cell therapies (idecabtagene vicleucel and ciltacabtagene autoleucel) as well as one BCMA/CD3 BsAb (teclistamab) have been approved for late-line (greater than four previous lines) R/R MM in the United States. The purpose of this review is to analyze the recent data for these approved therapies as well as provide an overview of other related CAR T-cell and BsAb therapies under development, including non-BCMA-targeting agents. We review efficacy and safety considerations, with particular focus on cytokine release syndrome, neurotoxicity, and infection risk. The relative merits and limitations of each class of therapy are discussed, as well as the areas of unmet need with respect to optimal sequencing and supportive care measures. We examine the factors that challenge equitable access to these novel therapies across minoritized racial, ethnic, and socioeconomic populations. Although it is evident that CAR T-cell and BsAb therapies will transform treatment paradigms in MM for years to come, significant work remains to identify the optimal utilization of these novel therapies and ensure equitable access.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
References
-
- Bal S, Malek E, Kansagra A, et al. : Treatment outcomes of triple class refractory multiple myeloma: A benchmark for new therapies. Leukemia 36:877-880, 2022 - PubMed
-
- Chari A, Vogl DT, Gavriatopoulou M, et al. : Oral selinexor-dexamethasone for triple-class refractory multiple myeloma. N Engl J Med 381:727-738, 2019 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
