

Redefining attrition in multiple myeloma (MM): a Canadian Myeloma Research Group (CMRG) analysis
- PMID: 37474492
- PMCID: PMC10359388
- DOI: 10.1038/s41408-023-00883-x
Redefining attrition in multiple myeloma (MM): a Canadian Myeloma Research Group (CMRG) analysis
Erratum in
-
Correction: Redefining attrition in multiple myeloma (MM): a Canadian Myeloma Research Group (CMRG) analysis.Blood Cancer J. 2023 Aug 28;13(1):129. doi: 10.1038/s41408-023-00888-6. Blood Cancer J. 2023. PMID: 37635183 Free PMC article. No abstract available.
Abstract
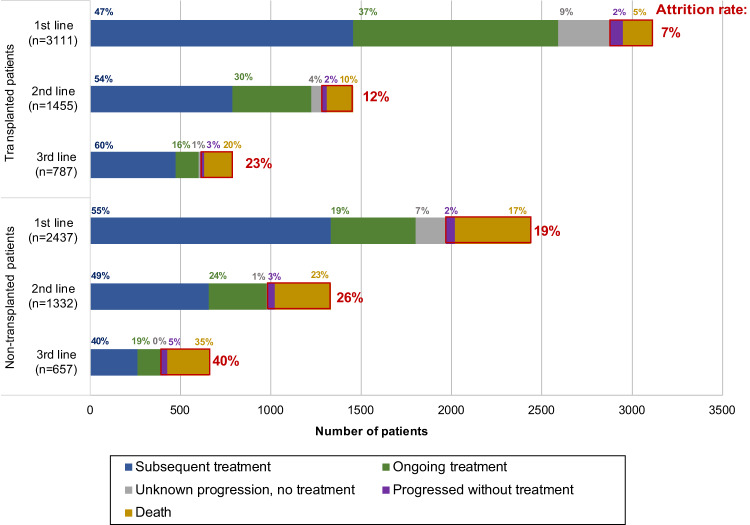
While most patients diagnosed with multiple myeloma (MM) receive initial therapy, reported attrition rates are high. Understanding attrition rates and characteristics of patients not receiving subsequent therapy is useful for MM stakeholders. We performed an analysis of attrition rates in a large disease-specific database of patients with newly diagnosed MM who received at least one line of therapy between Jan 1/10-Dec 31/20. Attrition was defined as failure to receive a subsequent line of therapy despite progression of MM or due to death. A total of 5548 patients were identified, 3111 autologous stem cell transplant (ASCT) patients and 2437 non-ASCT. In the ASCT cohort, the attrition rate was 7% after line 1, 12% after line 2, and 23% after line 3. In non-ASCT patients, the attrition rate was 19% after line 1, 26% after line 2, and 40% after line 3. Death was the dominant contributor to attrition across all cohorts, with a minority of patients alive with progressive disease in the absence of further therapy at each line. Multivariable analysis identified older age, shorter time to progression, and inferior response as independent risk factors for attrition. Our data show that attrition rates increase with each line of therapy and are higher in non-ASCT patients but are appreciably lower than previously reported. This study supports a revision of the previous definition of attrition, demonstrating that most patients who do not receive subsequent therapy are either continuing their current therapy and/or are in remission off-treatment rather than being irreversibly lost to attrition.
© 2023. The Author(s).
Conflict of interest statement
AM: Honoraria/Advisory fees: GSK, Janssen, BMS/Celgene, Forus therapeutics, Amgen, Takeda, Sanofi; research funding: BMS. HM: Honoraria/Advisory fees: GSK, Janssen, BMS/Celgene, Forus therapeutics, Amgen, Takeda, Sanofi; research funding: Janssen. RL: Honoraria/Advisory fees: Janssen, BMS, Amgen, Sanofi, Forus therapeutics. JS, EM-K, AR, MA, DB, and EG: None. AV: Honoraria/Advisory fees: Sanofi, Janssen, Apotex, Pfizer. ML: Honoraria: Janssen, BMS, Amgen and Pfizer. DW: Honoraria: Amgen, Antengene, BMS, Janssen, Karyopharm, Sanofi and Takeda. MS: Membership on an entity’s Board of Directors or advisory committees: Janssen Inc.; Amgen Canada; Takeda Canada; BMS Canada. RK: Research funding: Merck, Sanofi. Ownership/Share holder: Karyopharm. Honoraria: BMS, Janssen, Takeda, Amgen, Sanofi, Merck. DR: Honoraria/Advisory fees: BMS/Celgene, Janssen, Amgen, GSK, Sanofi, Forus Therapeutics, Takeda; research support: Jansen, BMS/Celgene, Takeda, Sanofi. CV: Honoraria: Janssen, Amgen, Takeda; research funding: BMS, Amgen. VJZ: Honoraria: Janssen, BMS/Celgene, Takeda, AMGEN, Forus therapeutics, Pfizer, Sanofi, GSK.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
