

The copy number and mutational landscape of recurrent ovarian high-grade serous carcinoma
- PMID: 37474499
- PMCID: PMC10359414
- DOI: 10.1038/s41467-023-39867-7
The copy number and mutational landscape of recurrent ovarian high-grade serous carcinoma
Erratum in
-
Author Correction: The copy number and mutational landscape of recurrent ovarian high-grade serous carcinoma.Nat Commun. 2023 Sep 26;14(1):5992. doi: 10.1038/s41467-023-41611-0. Nat Commun. 2023. PMID: 37752102 Free PMC article. No abstract available.
Abstract
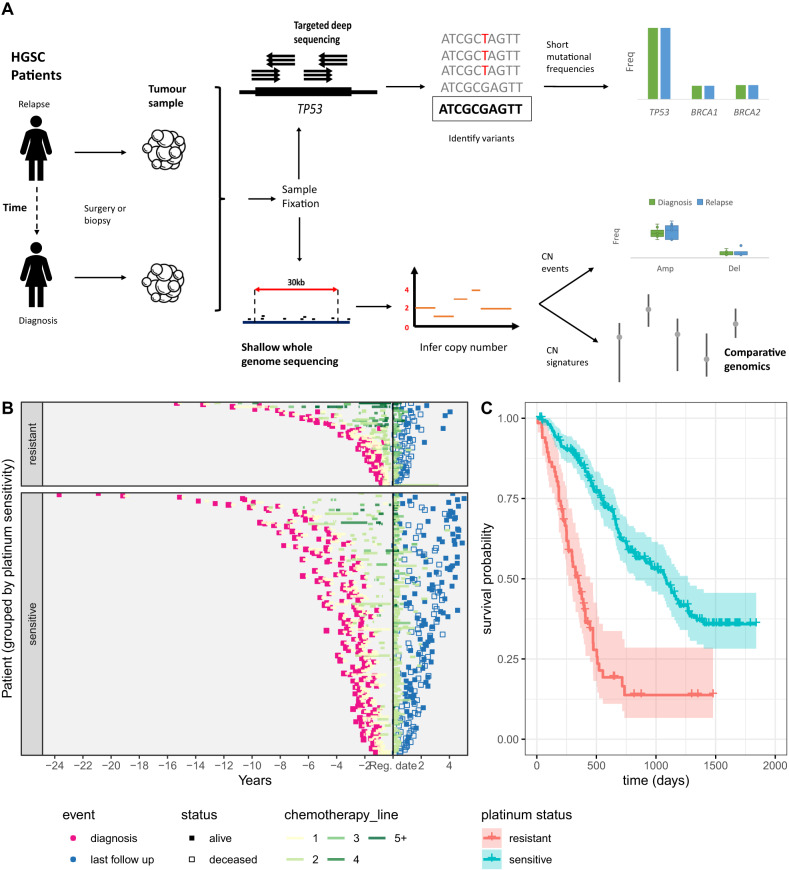
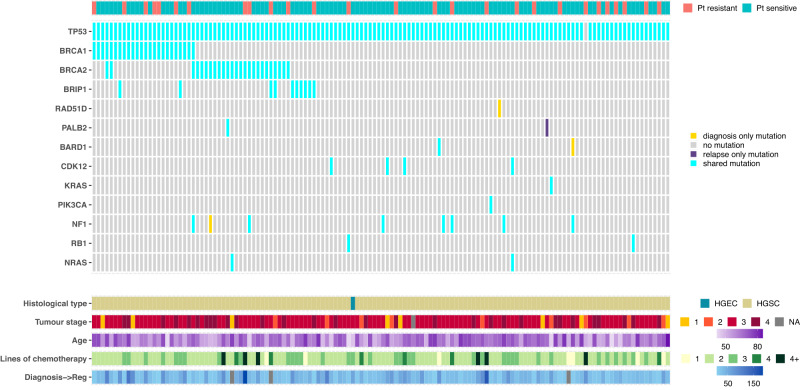
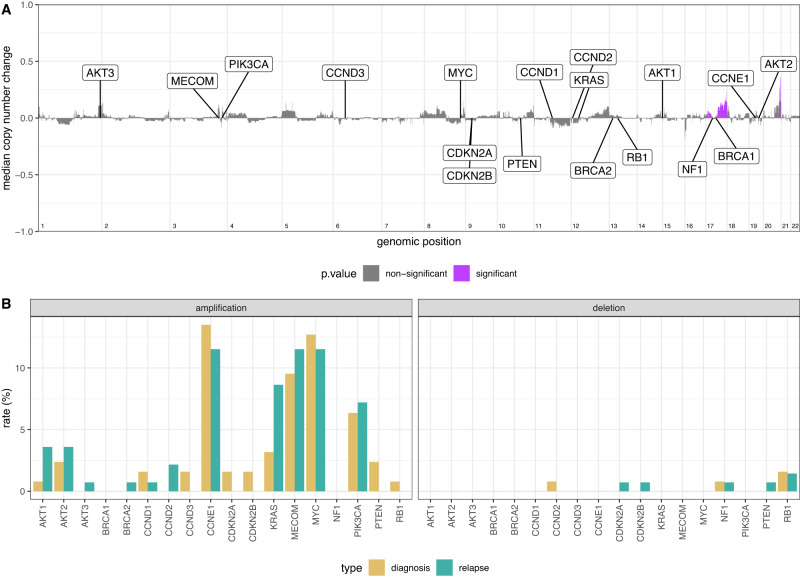
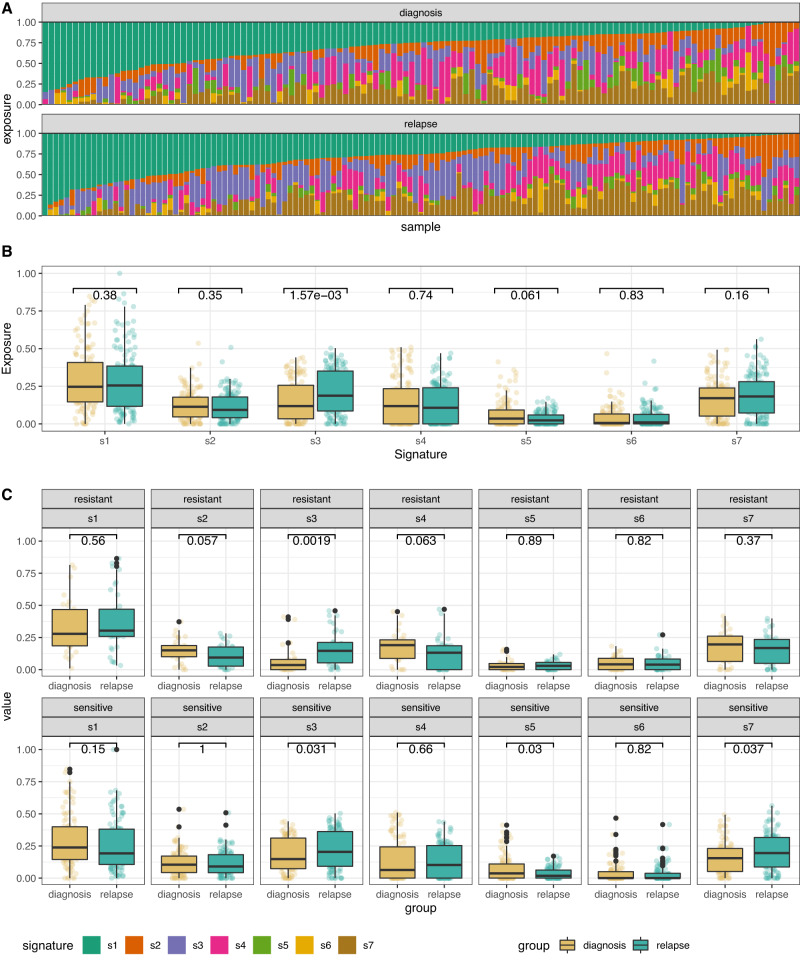
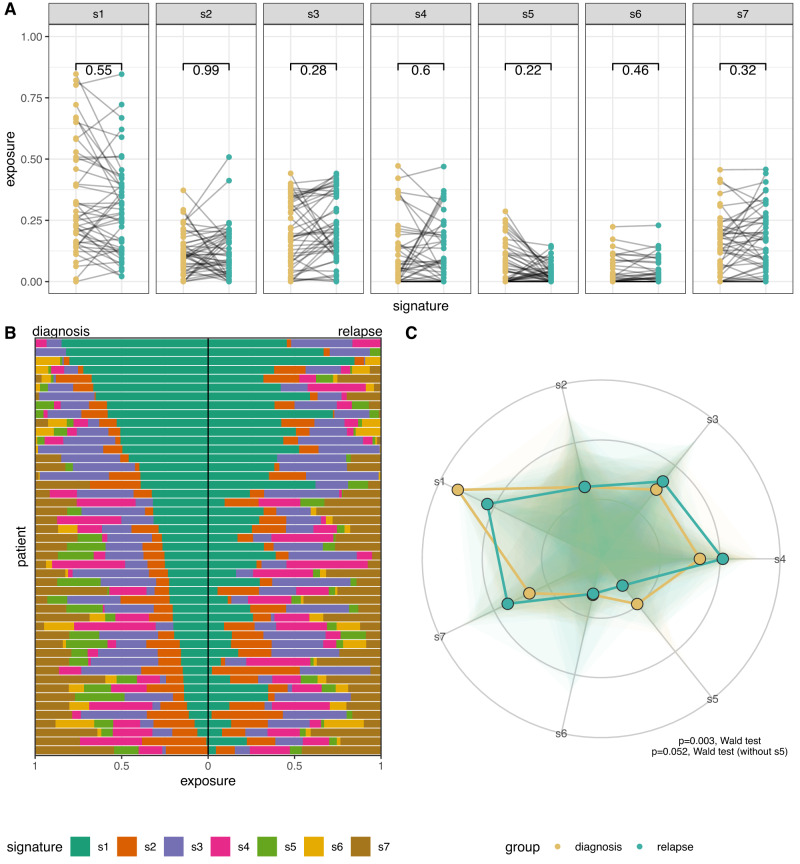
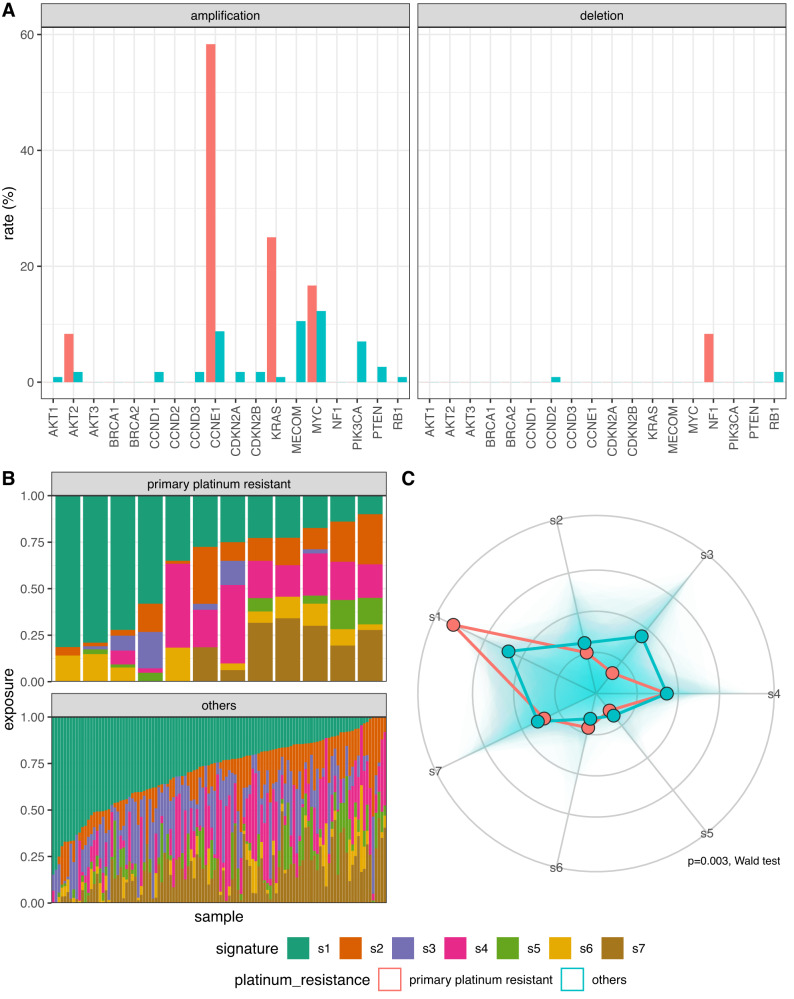
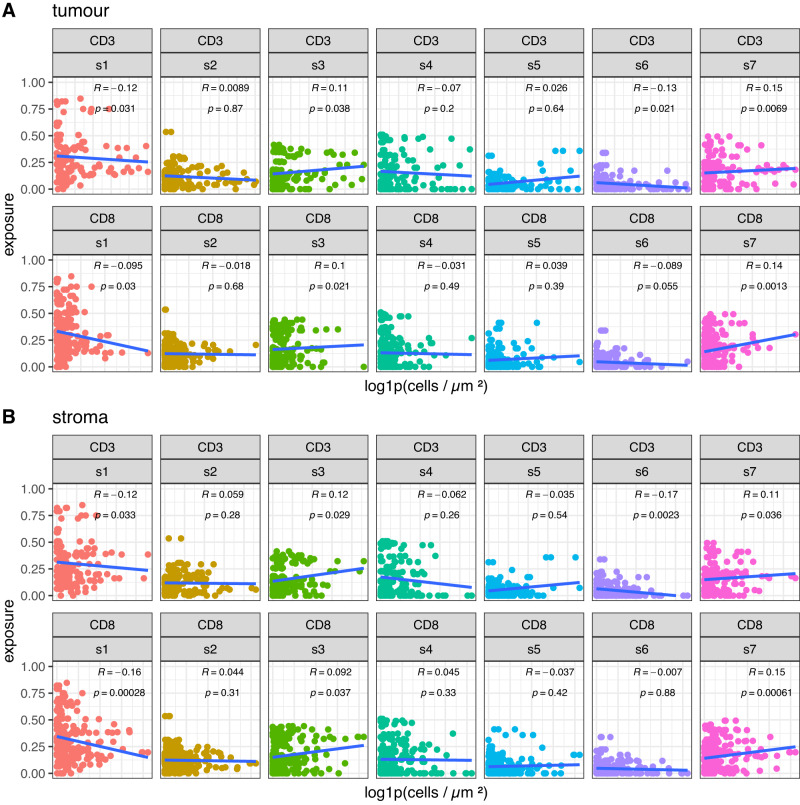
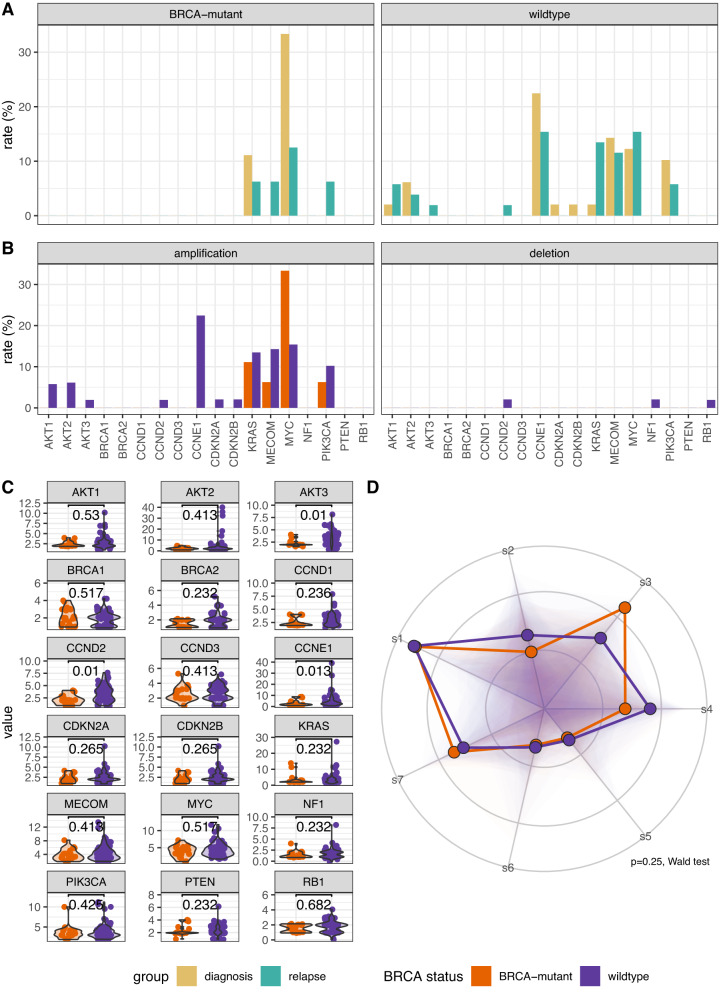
The drivers of recurrence and resistance in ovarian high grade serous carcinoma remain unclear. We investigate the acquisition of resistance by collecting tumour biopsies from a cohort of 276 women with relapsed ovarian high grade serous carcinoma in the BriTROC-1 study. Panel sequencing shows close concordance between diagnosis and relapse, with only four discordant cases. There is also very strong concordance in copy number between diagnosis and relapse, with no significant difference in purity, ploidy or focal somatic copy number alterations, even when stratified by platinum sensitivity or prior chemotherapy lines. Copy number signatures are strongly correlated with immune cell infiltration, whilst diagnosis samples from patients with primary platinum resistance have increased rates of CCNE1 and KRAS amplification and copy number signature 1 exposure. Our data show that the ovarian high grade serous carcinoma genome is remarkably stable between diagnosis and relapse and acquired chemotherapy resistance does not select for common copy number drivers.
© 2023. The Author(s).
Conflict of interest statement
G.M., F.M., A.M.P. and J.D.B. are founders and shareholders of Tailor Bio Ltd. The remaining authors declare no competing interests.
Figures
References
-
- Gorringe KL, et al. High-resolution single nucleotide polymorphism array analysis of epithelial ovarian cancer reveals numerous microdeletions and amplifications. Clin. Cancer Res. 2007;13:4731–4739. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
