

Predicting sepsis onset using a machine learned causal probabilistic network algorithm based on electronic health records data
- PMID: 37474597
- PMCID: PMC10359402
- DOI: 10.1038/s41598-023-38858-4
Predicting sepsis onset using a machine learned causal probabilistic network algorithm based on electronic health records data
Abstract
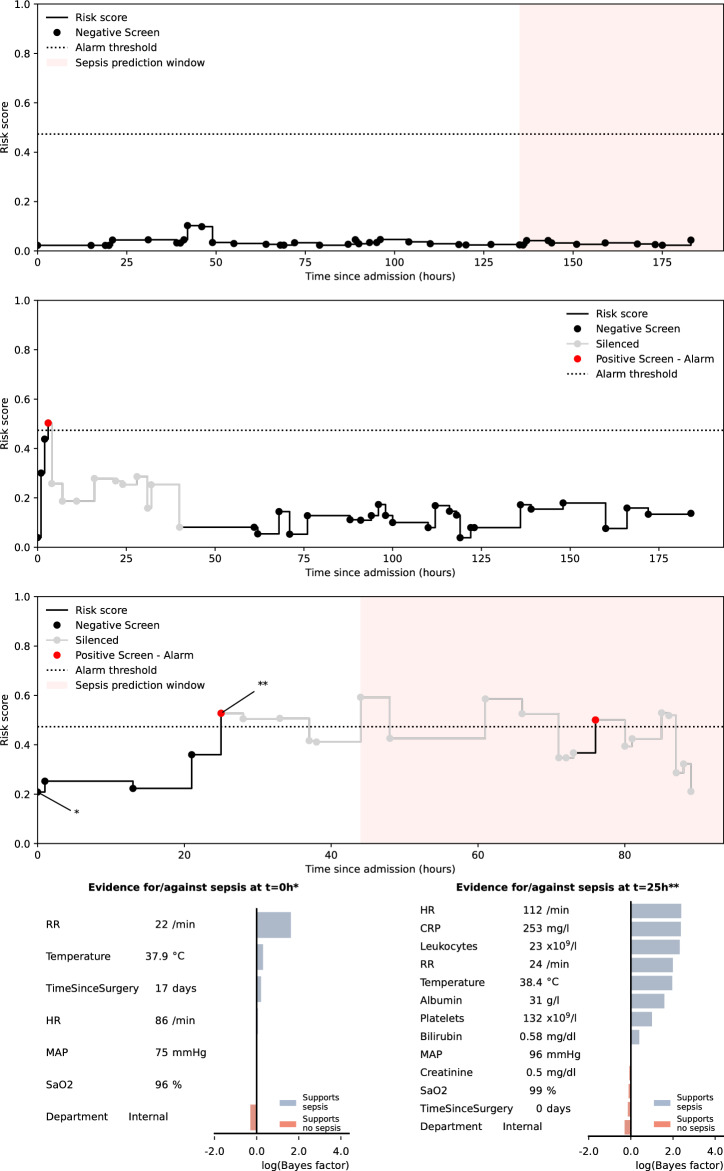
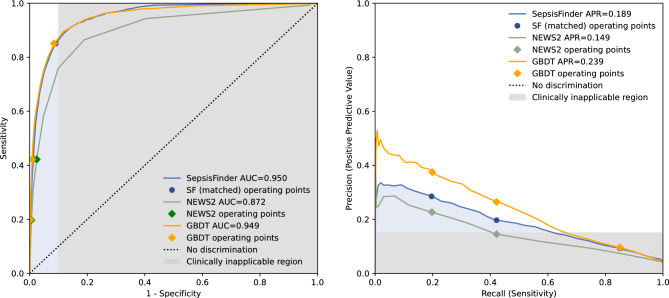
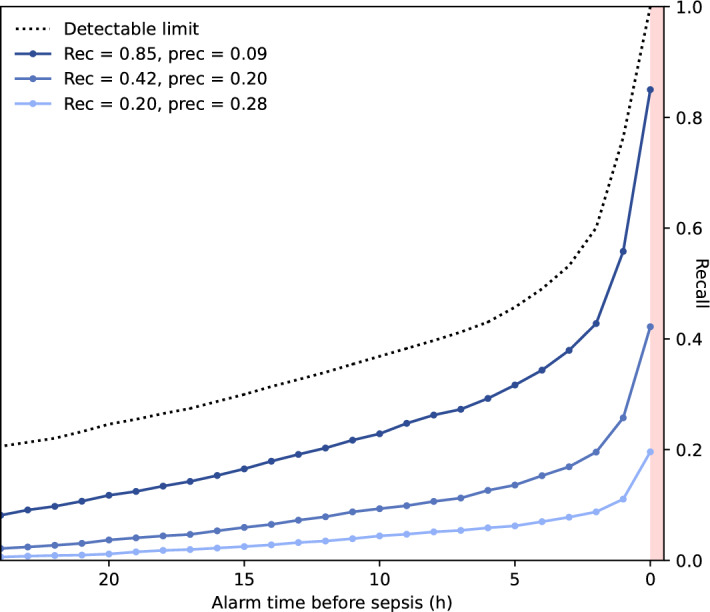
Sepsis is a leading cause of mortality and early identification improves survival. With increasing digitalization of health care data automated sepsis prediction models hold promise to aid in prompt recognition. Most previous studies have focused on the intensive care unit (ICU) setting. Yet only a small proportion of sepsis develops in the ICU and there is an apparent clinical benefit to identify patients earlier in the disease trajectory. In this cohort of 82,852 hospital admissions and 8038 sepsis episodes classified according to the Sepsis-3 criteria, we demonstrate that a machine learned score can predict sepsis onset within 48 h using sparse routine electronic health record data outside the ICU. Our score was based on a causal probabilistic network model-SepsisFinder-which has similarities with clinical reasoning. A prediction was generated hourly on all admissions, providing a new variable was registered. Compared to the National Early Warning Score (NEWS2), which is an established method to identify sepsis, the SepsisFinder triggered earlier and had a higher area under receiver operating characteristic curve (AUROC) (0.950 vs. 0.872), as well as area under precision-recall curve (APR) (0.189 vs. 0.149). A machine learning comparator based on a gradient-boosting decision tree model had similar AUROC (0.949) and higher APR (0.239) than SepsisFinder but triggered later than both NEWS2 and SepsisFinder. The precision of SepsisFinder increased if screening was restricted to the earlier admission period and in episodes with bloodstream infection. Furthermore, the SepsisFinder signaled median 5.5 h prior to antibiotic administration. Identifying a high-risk population with this method could be used to tailor clinical interventions and improve patient care.
© 2023. The Author(s).
Conflict of interest statement
LW and MLM are employees of Treat Systems ApS (Aalborg, Denmark) and owns shares in the company. Treat Systems produces medical decision support systems for antimicrobial and microbiological diagnostic stewardship, however SepsisFinder is currently not used for the purpose of sepsis screening. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
