

Mitigating neurological, cognitive, and psychiatric sequelae of COVID-19-related critical illness
- PMID: 37475124
- PMCID: PMC10706757
- DOI: 10.1016/S2213-2600(23)00238-2
Mitigating neurological, cognitive, and psychiatric sequelae of COVID-19-related critical illness
Abstract
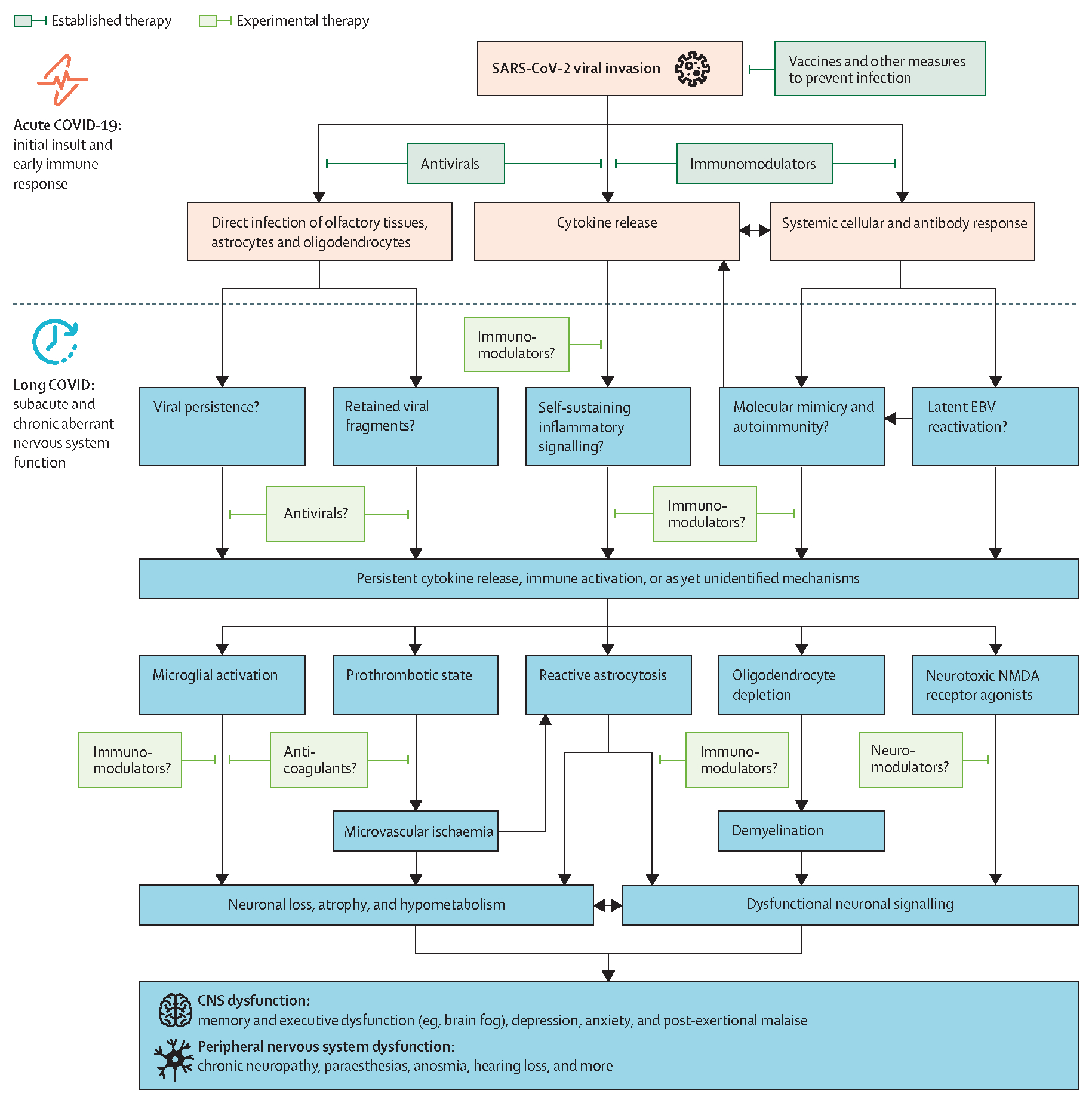
Despite advances in the treatment and mitigation of critical illness caused by infection with SARS-CoV-2, millions of survivors have a devastating, post-acute infection syndrome known as long COVID. A large proportion of patients with long COVID have nervous system dysfunction, which is also seen in the distinct but overlapping condition of post-intensive care syndrome (PICS), putting survivors of COVID-19-related critical illness at high risk of long-lasting morbidity affecting multiple organ systems and, as a result, engendering measurable deficits in quality of life and productivity. In this Series paper, we discuss neurological, cognitive, and psychiatric sequelae in patients who have survived critical illness due to COVID-19. We review current knowledge of the epidemiology and pathophysiology of persistent neuropsychological impairments, and outline potential preventive strategies based on safe, evidence-based approaches to the management of pain, agitation, delirium, anticoagulation, and ventilator weaning during critical illness. We highlight priorities for current and future research, including possible therapeutic approaches, and offer considerations for health services to address the escalating health burden of long COVID.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests EWE and SWR have submitted a grant proposal to study the effects of baricitinib on long COVID. The other authors declare no competing interests.
Figures

Comment in
-
Long COVID-unravelling a complex condition.Lancet Respir Med. 2023 Aug;11(8):667-668. doi: 10.1016/S2213-2600(23)00232-1. Epub 2023 Jul 17. Lancet Respir Med. 2023. PMID: 37475126 No abstract available.
References
-
- WHO. WHO Coronavirus (COVID-19) Dashboard. 2023. https://covid19.who.int (accessed July 1, 2023).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
