

Three-dimensional endovaginal ultrasound assessment using the levator ani deficiency score in primiparas: A replication study
- PMID: 37475151
- PMCID: PMC10407012
- DOI: 10.1111/aogs.14633
Three-dimensional endovaginal ultrasound assessment using the levator ani deficiency score in primiparas: A replication study
Abstract
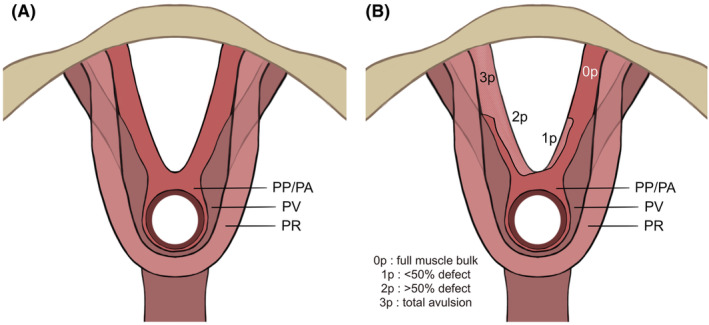
Introduction: It is essential to assess the levator ani properly as part of clinical care in patients presenting with pelvic floor dysfunction. The levator ani deficiency scoring system is a previously published method to assess levator ani defects with three-dimensional endovaginal ultrasound. The primary aim of this study was to determine the intra- and interrater reliability of the levator ani deficiency score in a cohort of non-instrumentally delivered primiparas.
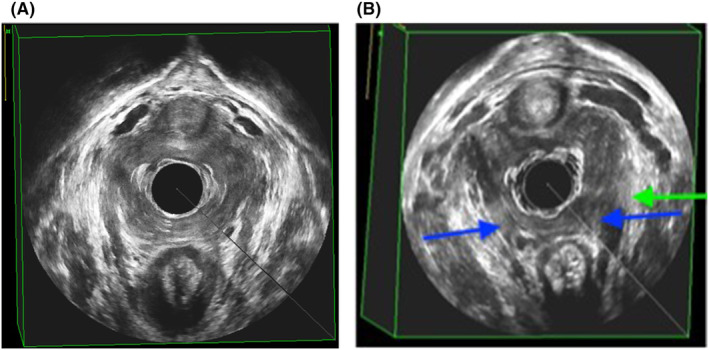
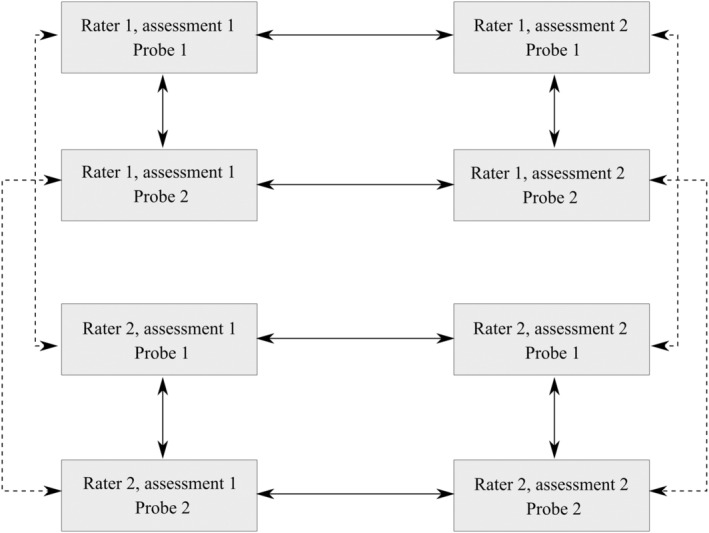
Material and methods: Primiparas (n = 141) were examined at least 1 year after vaginal birth. Three-dimensional endovaginal ultrasound volumes were acquired by a single examiner using two different automated ultrasound probes. The volumes were analyzed by two separate raters who were blinded to each other's assessments. Descriptive statistics were calculated for levator ani deficiency score and categorized into three levels (mild, moderate, severe). Kendall's tau-b was calculated for intra- and interrater comparisons.
Results: Intrarater comparisons of levator ani deficiency score and levator ani deficiency category were high (Kendall's tau-b ≥0.80 for Rater 1; >0.79 for Rater 2). Interrater comparisons of levator ani deficiency score and levator ani deficiency category were also high (Kendall's tau-b >0.9 for assessment 1 and >0.78 for assessment 2). Varying by rater, probe and assessment, 75.9%-80.1% of the study population had no/mild deficiency, 6.4%-9.2% had moderate deficiency, and 4.3%-6.4% had severe levator ani deficiency.
Conclusions: The levator ani deficiency scoring system is a feasible method to assess defects of the levator ani muscle and can be reproduced with high intra- and interrater correlations. Using the scoring system in clinical practice may facilitate concordant assessment between different examiners. However, the system should be used to support clinical findings and symptomatology and not as a screening tool, as the score is lacking the category of no levator ani deficiency.
Keywords: levator ani avulsion; levator ani muscle; pelvic floor dysfunction; systematic scoring; ultrasound; vaginal birth.
© 2023 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Figures
References
-
- Shek KL, Dietz HP. Intrapartum risk factors for levator trauma. BJOG. 2010;117:1485‐1492. - PubMed
-
- Dietz HP. Pelvic floor trauma in childbirth. Aust N Z J Obstet Gynaecol. 2013;53:220‐230. - PubMed
-
- Dietz HP, Chantarasorn V, Shek KL. Levator avulsion is a risk factor for cystocele recurrence. Ultrasound Obstet Gynecol. 2010;36:76‐80. - PubMed
-
- Chantarasorn V, Shek KL, Dietz HP. Sonographic detection of puborectalis muscle avulsion is not associated with anal incontinence. Aust N Z J Obstet Gynaecol. 2011;51:130‐135. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
