

Investigation of autosegmentation techniques on T2-weighted MRI for off-line dose reconstruction in MR-linac workflow for head and neck cancers
- PMID: 37475466
- PMCID: PMC10799175
- DOI: 10.1002/mp.16582
Investigation of autosegmentation techniques on T2-weighted MRI for off-line dose reconstruction in MR-linac workflow for head and neck cancers
Abstract
Background: In order to accurately accumulate delivered dose for head and neck cancer patients treated with the Adapt to Position workflow on the 1.5T magnetic resonance imaging (MRI)-linear accelerator (MR-linac), the low-resolution T2-weighted MRIs used for daily setup must be segmented to enable reconstruction of the delivered dose at each fraction.
Purpose: In this pilot study, we evaluate various autosegmentation methods for head and neck organs at risk (OARs) on on-board setup MRIs from the MR-linac for off-line reconstruction of delivered dose.
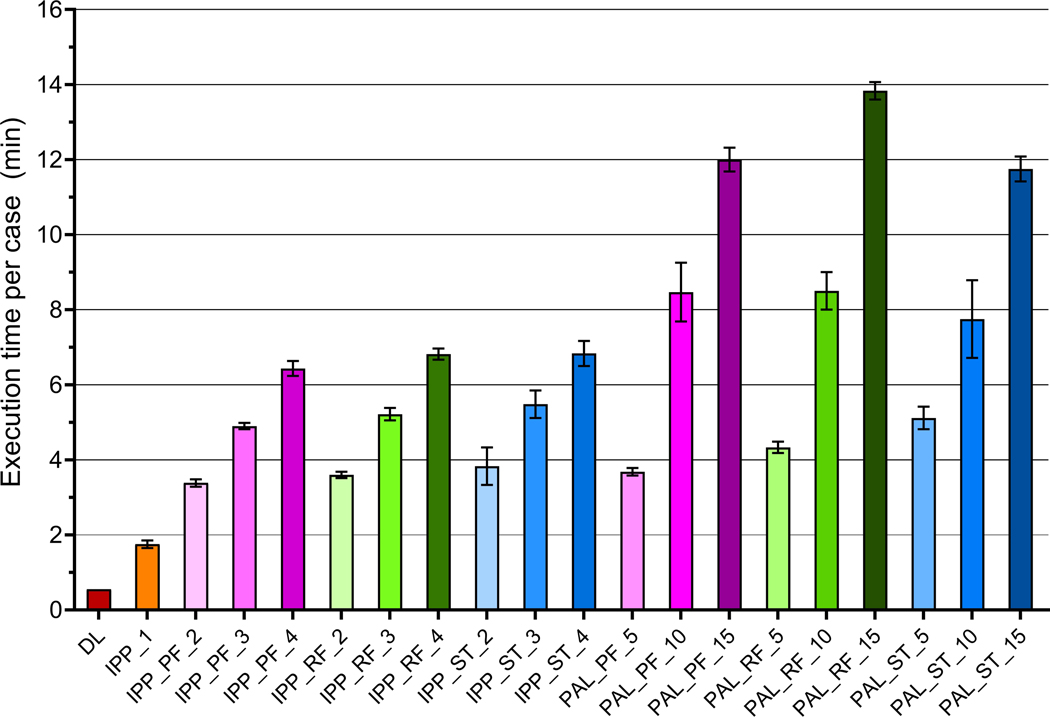
Methods: Seven OARs (parotid glands, submandibular glands, mandible, spinal cord, and brainstem) were contoured on 43 images by seven observers each. Ground truth contours were generated using a simultaneous truth and performance level estimation (STAPLE) algorithm. Twenty total autosegmentation methods were evaluated in ADMIRE: 1-9) atlas-based autosegmentation using a population atlas library (PAL) of 5/10/15 patients with STAPLE, patch fusion (PF), random forest (RF) for label fusion; 10-19) autosegmentation using images from a patient's 1-4 prior fractions (individualized patient prior [IPP]) using STAPLE/PF/RF; 20) deep learning (DL) (3D ResUNet trained on 43 ground truth structure sets plus 45 contoured by one observer). Execution time was measured for each method. Autosegmented structures were compared to ground truth structures using the Dice similarity coefficient, mean surface distance (MSD), Hausdorff distance (HD), and Jaccard index (JI). For each metric and OAR, performance was compared to the inter-observer variability using Dunn's test with control. Methods were compared pairwise using the Steel-Dwass test for each metric pooled across all OARs. Further dosimetric analysis was performed on three high-performing autosegmentation methods (DL, IPP with RF and 4 fractions [IPP_RF_4], IPP with 1 fraction [IPP_1]), and one low-performing (PAL with STAPLE and 5 atlases [PAL_ST_5]). For five patients, delivered doses from clinical plans were recalculated on setup images with ground truth and autosegmented structure sets. Differences in maximum and mean dose to each structure between the ground truth and autosegmented structures were calculated and correlated with geometric metrics.
Results: DL and IPP methods performed best overall, all significantly outperforming inter-observer variability and with no significant difference between methods in pairwise comparison. PAL methods performed worst overall; most were not significantly different from the inter-observer variability or from each other. DL was the fastest method (33 s per case) and PAL methods the slowest (3.7-13.8 min per case). Execution time increased with a number of prior fractions/atlases for IPP and PAL. For DL, IPP_1, and IPP_RF_4, the majority (95%) of dose differences were within ± 250 cGy from ground truth, but outlier differences up to 785 cGy occurred. Dose differences were much higher for PAL_ST_5, with outlier differences up to 1920 cGy. Dose differences showed weak but significant correlations with all geometric metrics (R2 between 0.030 and 0.314).
Conclusions: The autosegmentation methods offering the best combination of performance and execution time are DL and IPP_1. Dose reconstruction on on-board T2-weighted MRIs is feasible with autosegmented structures with minimal dosimetric variation from ground truth, but contours should be visually inspected prior to dose reconstruction in an end-to-end dose accumulation workflow.
Keywords: MR-linac; autosegmentation; head and neck cancers.
© 2023 The Authors. Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
Conflict of Interest Statement
The remaining authors have no conflicts of interest to disclose.
Figures





Similar articles
-
Geometric and dosimetric evaluations of atlas-based segmentation methods of MR images in the head and neck region.Phys Med Biol. 2018 Jul 11;63(14):145007. doi: 10.1088/1361-6560/aacb65. Phys Med Biol. 2018. PMID: 29882749 Free PMC article.
-
vOARiability: Interobserver and intermodality variability analysis in OAR contouring from head and neck CT and MR images.Med Phys. 2024 Mar;51(3):2175-2186. doi: 10.1002/mp.16924. Epub 2024 Jan 17. Med Phys. 2024. PMID: 38230752
-
Clinical validation of atlas-based auto-segmentation of multiple target volumes and normal tissue (swallowing/mastication) structures in the head and neck.Int J Radiat Oncol Biol Phys. 2011 Nov 15;81(4):950-7. doi: 10.1016/j.ijrobp.2010.07.009. Epub 2010 Oct 6. Int J Radiat Oncol Biol Phys. 2011. PMID: 20932664
-
Auto-segmentation of organs at risk for head and neck radiotherapy planning: From atlas-based to deep learning methods.Med Phys. 2020 Sep;47(9):e929-e950. doi: 10.1002/mp.14320. Epub 2020 Jul 28. Med Phys. 2020. PMID: 32510603 Review.
-
Automated segmentation in planning-CT for breast cancer radiotherapy: A review of recent advances.Radiother Oncol. 2025 Jan;202:110615. doi: 10.1016/j.radonc.2024.110615. Epub 2024 Nov 1. Radiother Oncol. 2025. PMID: 39489430 Review.
Cited by
-
Deep-learning-based generation of synthetic 6-minute MRI from 2-minute MRI for use in head and neck cancer radiotherapy.Front Oncol. 2022 Nov 8;12:975902. doi: 10.3389/fonc.2022.975902. eCollection 2022. Front Oncol. 2022. PMID: 36425548 Free PMC article.
-
Evaluation of deep learning-based multiparametric MRI oropharyngeal primary tumor auto-segmentation and investigation of input channel effects: Results from a prospective imaging registry.Clin Transl Radiat Oncol. 2021 Oct 16;32:6-14. doi: 10.1016/j.ctro.2021.10.003. eCollection 2022 Jan. Clin Transl Radiat Oncol. 2021. PMID: 34765748 Free PMC article.
-
Comparing multi-image and image augmentation strategies for deep learning-based prostate segmentation.Phys Imaging Radiat Oncol. 2024 Feb 20;29:100551. doi: 10.1016/j.phro.2024.100551. eCollection 2024 Jan. Phys Imaging Radiat Oncol. 2024. PMID: 38444888 Free PMC article.
-
Application of simultaneous uncertainty quantification for image segmentation with probabilistic deep learning: Performance benchmarking of oropharyngeal cancer target delineation as a use-case.medRxiv [Preprint]. 2023 Feb 24:2023.02.20.23286188. doi: 10.1101/2023.02.20.23286188. medRxiv. 2023. PMID: 36865296 Free PMC article. Preprint.
-
Segmentation stability of human head and neck cancer medical images for radiotherapy applications under de-identification conditions: Benchmarking data sharing and artificial intelligence use-cases.Front Oncol. 2023 Feb 28;13:1120392. doi: 10.3389/fonc.2023.1120392. eCollection 2023. Front Oncol. 2023. PMID: 36925936 Free PMC article.
References
-
- McDonald BA, Vedam S, Yang J, et al. Initial Feasibility and Clinical Implementation of Daily MR-Guided Adaptive Head and Neck Cancer Radiation Therapy on a 1.5T MR-Linac System: Prospective R-IDEAL 2a/2b Systematic Clinical Evaluation of Technical Innovation. Int J Radiat Oncol. 2021;109(5):1606–1618. doi:10.1016/j.ijrobp.2020.12.015 - DOI - PMC - PubMed
MeSH terms
Grants and funding
- T32 CA261856/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
- F31 DE029093/DE/NIDCR NIH HHS/United States
- R01 DE025248/DE/NIDCR NIH HHS/United States
- R01 CA214825/CA/NCI NIH HHS/United States
- R25 EB025787/EB/NIBIB NIH HHS/United States
- R56 DE025248/DE/NIDCR NIH HHS/United States
- R01 CA218148/CA/NCI NIH HHS/United States
- R01 CA225190/CA/NCI NIH HHS/United States
- PCS-1609-36195/PCORI/Patient-Centered Outcomes Research Institute/United States
- F31 DE031502/DE/NIDCR NIH HHS/United States
- P50 CA097007/CA/NCI NIH HHS/United States
- R01 DE028290/DE/NIDCR NIH HHS/United States
- TL1 TR003169/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
