

The effect of restrictive fluid management on outcomes among geriatric hip fractures: a retrospective cohort study at five level I trauma centers
- PMID: 37475886
- PMCID: PMC10356122
- DOI: 10.1097/OI9.0000000000000279
The effect of restrictive fluid management on outcomes among geriatric hip fractures: a retrospective cohort study at five level I trauma centers
Abstract
Restrictive fluid management (RFM) for hemodynamically unstable trauma patients has reduced mortality rates. The objective was to determine whether RFM benefits geriatric hip fracture patients, who are usually hemodynamically stable.
Design: Retrospective propensity-matched study.
Setting: Five Level I trauma centers (January 1, 2018-December 12, 2018).
Patients: Geriatric patients (65 years or older) with hip fractures were included in this study. Patients with multiple injuries, nonoperative management, and preoperative blood products were excluded.
Intervention: Patients were grouped by fluid volume (normal saline, lactated Ringer, dextrose, electrolytes, and medications) received preoperatively or ≤24 hours of arrival; patients with standard fluid management (SFM) received ≥150 mL and RFM <150 mL of fluids.
Main outcome measurements: The primary outcomes were length of stay (LOS), delayed ambulation (>2 days postoperatively), and mortality. Paired Student t-tests, Wilcoxon paired rank sum tests, and McNemar tests were used; an α value of < 0.05 was considered statistically significant.
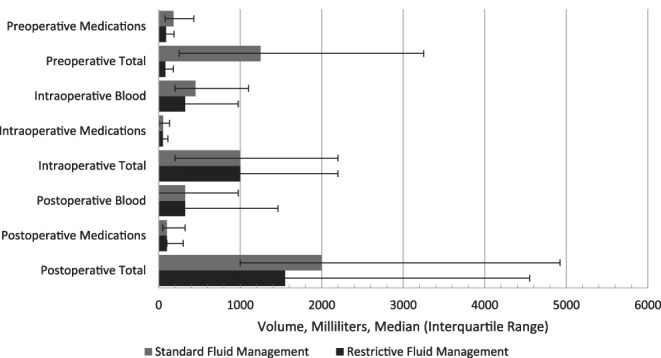
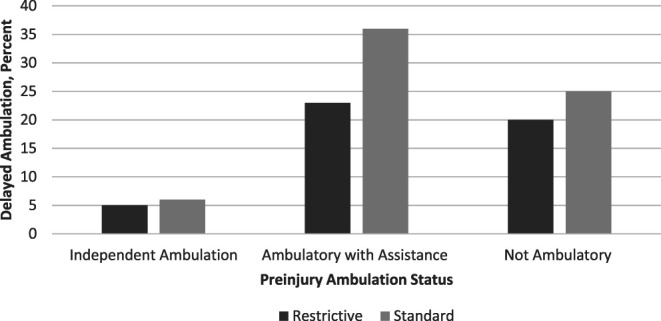
Results: There were 523 patients (40% RFM, 60% SFM); after matching, there were 95 patients per arm. The matched patients were well-balanced, including no difference in time from arrival to surgery. RFM and SFM patients received a median of 80 mL and 1250 mL of preoperative fluids, respectively (P < 0.001). Postoperative fluid volumes were 1550 versus 2000 mL, respectively, (P = 0.73), and LOSs were similar between the two groups (5 versus 5 days, P = 0.83). Mortality and complications, including acute kidney injuries, were similar. Delayed ambulation rates were similar overall. When stratified by preinjury ambulation status, SFM was associated with delayed ambulation for patients not walking independently before injury (P = 0.01), but RFM was not (P = 0.09).
Conclusions: RFM seems to be safe in terms of laboratory results, complications, and disposition. SFM may lead to delayed ambulation for patients who are not walking independently before injury.
Keywords: geriatric trauma; hip fracture; restrictive fluid management; resuscitation.
Copyright © 2023 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Orthopaedic Trauma Association.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Significant variations in preoperative fluid resuscitation volumes delivered to elderly hip fracture patients at six level 1 trauma centers: an observational descriptive study.OTA Int. 2022 Jan 3;5(1):e162. doi: 10.1097/OI9.0000000000000162. eCollection 2022 Mar. OTA Int. 2022. PMID: 34984321 Free PMC article.
-
Improving community ambulation after hip fracture: protocol for a randomised, controlled trial.J Physiother. 2017 Jan;63(1):45-46. doi: 10.1016/j.jphys.2016.10.001. Epub 2016 Oct 28. J Physiother. 2017. PMID: 27964962 Free PMC article. Clinical Trial.
-
Is Delayed Time to Surgery Associated with Increased Short-term Complications in Patients with Pathologic Hip Fractures?Clin Orthop Relat Res. 2020 Mar;478(3):607-615. doi: 10.1097/CORR.0000000000001038. Clin Orthop Relat Res. 2020. PMID: 31702689 Free PMC article.
-
Does Care at a Trauma Center Affect Geriatric Hip Fracture Patients?Geriatr Orthop Surg Rehabil. 2020 Mar 16;11:2151459320911865. doi: 10.1177/2151459320911865. eCollection 2020. Geriatr Orthop Surg Rehabil. 2020. PMID: 32206383 Free PMC article.
-
Elderly adults with isolated hip fractures- orthogeriatric care versus standard care: A practice management guideline from the Eastern Association for the Surgery of Trauma.J Trauma Acute Care Surg. 2020 Feb;88(2):266-278. doi: 10.1097/TA.0000000000002482. J Trauma Acute Care Surg. 2020. PMID: 31464870
References
-
- American College of Surgeons; The Committee on Trauma. Advanced Trauma Life Support® Tenth Edition. American College of Surgeons; Chicago, IL; 2018.
-
- Duke MD, Guidry C, Guice J, et al. Restrictive fluid resuscitation in combination with damage control resuscitation: time for adaptation. J Trauma Acute Care Surg. 2012;73:674–678. - PubMed
-
- Karcioglu O. Permissive hypotension: what's new in fluid resuscitation in the management of hemorrhagic shock? J Anesth Intensive Care Med. 2018;7:555708.
LinkOut - more resources
Full Text Sources