

Metronomic Administration of Topotecan Alone and in Combination with Docetaxel Inhibits Epithelial-mesenchymal Transition in Aggressive Variant Prostate Cancers
- PMID: 37476073
- PMCID: PMC10355222
- DOI: 10.1158/2767-9764.CRC-22-0427
Metronomic Administration of Topotecan Alone and in Combination with Docetaxel Inhibits Epithelial-mesenchymal Transition in Aggressive Variant Prostate Cancers
Abstract
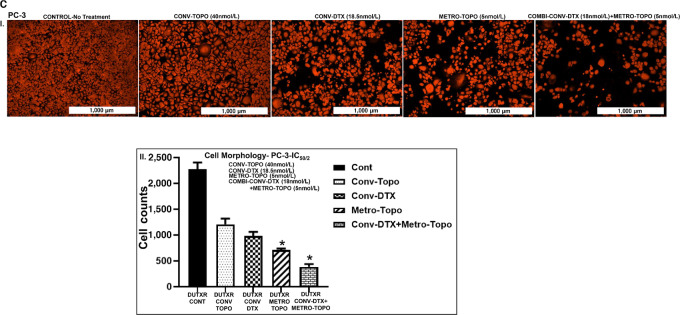
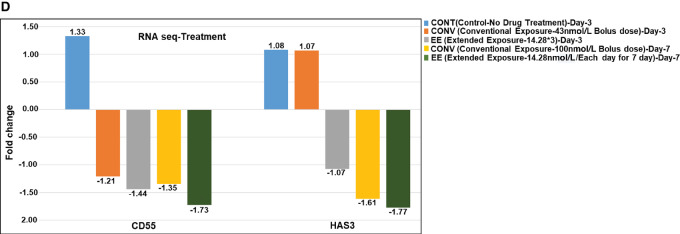
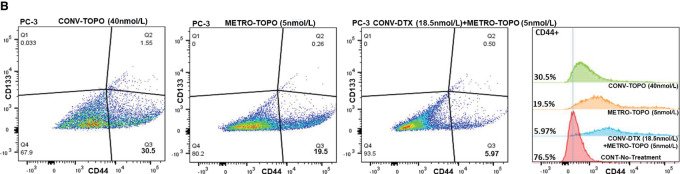
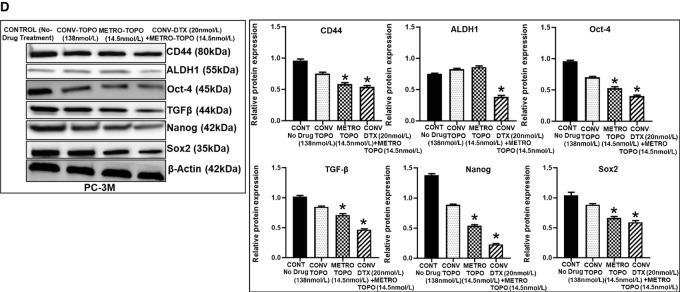
Prostate cancer is the second leading cause of noncutaneous cancer-related deaths in American men. Androgen deprivation therapy (ADT), radical prostatectomy, and radiotherapy remain the primary treatment for patients with early-stage prostate cancer (castration-sensitive prostate cancer). Following ADT, many patients ultimately develop metastatic castration-resistant prostate cancer (mCRPC). Standard chemotherapy options for CRPC are docetaxel (DTX) and cabazitaxel, which increase median survival, although the development of resistance is common. Cancer stem-like cells possess mesenchymal phenotypes [epithelial-to-mesenchymal transition (EMT)] and play crucial roles in tumor initiation and progression of mCRPC. We have shown that low-dose continuous administration of topotecan (METRO-TOPO) inhibits prostate cancer growth by interfering with key cancer pathway genes. This study utilized bulk and single-cell or whole-transcriptome analysis [(RNA sequencing (RNA-seq) and single-cell RNA sequencing (scRNA-seq)], and we observed greater expression of several EMT markers, including Vimentin, hyaluronan synthase-3, S100 calcium binding protein A6, TGFB1, CD44, CD55, and CD109 in European American and African American aggressive variant prostate cancer (AVPC) subtypes-mCRPC, neuroendocrine variant (NEPC), and taxane-resistant. The taxane-resistant gene FSCN1 was also expressed highly in single-cell subclonal populations in mCRPC. Furthermore, metronomic-topotecan single agent and combinations with DTX downregulated these EMT markers as well as CD44+ and CD44+/CD133+ "stem-like" cell populations. A microfluidic chip-based cell invasion assay revealed that METRO-TOPO treatment as a single agent or in combination with DTX was potentially effective against invasive prostate cancer spread. Our RNA-seq and scRNA-seq analysis were supported by in silico and in vitro studies, suggesting METRO-TOPO combined with DTX may inhibit oncogenic progression by reducing cancer stemness in AVPC through the inhibition of EMT markers and multiple oncogenic factors/pathways.
Significance: The utilization of metronomic-like dosing regimens of topotecan alone and in combination with DTX resulted in the suppression of makers associated with EMT and stem-like cell populations in AVPC models. The identification of molecular signatures and their potential to serve as novel biomarkers for monitoring treatment efficacy and disease progression response to treatment efficacy and disease progression were achieved using bulk RNA-seq and single-cell-omics methodologies.
© 2023 The Authors; Published by the American Association for Cancer Research.
Figures




















Similar articles
-
The Andrographolide Analogue 3A.1 Synergizes with Taxane Derivatives in Aggressive Metastatic Prostate Cancers by Upregulation of Heat Shock Proteins and Downregulation of MAT2A-Mediated Cell Migration and Invasion.J Pharmacol Exp Ther. 2022 Mar;380(3):180-201. doi: 10.1124/jpet.121.000898. Epub 2021 Dec 23. J Pharmacol Exp Ther. 2022. PMID: 34949650
-
Survival Outcomes of Concurrent Treatment with Docetaxel and Androgen Deprivation Therapy in Metastatic Castration-Resistant Prostate Cancer.Yonsei Med J. 2016 Sep;57(5):1070-8. doi: 10.3349/ymj.2016.57.5.1070. Yonsei Med J. 2016. PMID: 27401636 Free PMC article.
-
Androgen receptor negatively regulates mitotic checkpoint signaling to induce docetaxel resistance in castration-resistant prostate cancer.Prostate. 2022 Feb;82(2):182-192. doi: 10.1002/pros.24257. Epub 2021 Oct 21. Prostate. 2022. PMID: 34672379 Free PMC article.
-
Taxane-based Combination Therapies for Metastatic Prostate Cancer.Eur Urol Focus. 2019 May;5(3):369-380. doi: 10.1016/j.euf.2017.11.009. Epub 2017 Dec 21. Eur Urol Focus. 2019. PMID: 29275145 Review.
-
Exploitation of the Androgen Receptor to Overcome Taxane Resistance in Advanced Prostate Cancer.Adv Cancer Res. 2015;127:123-58. doi: 10.1016/bs.acr.2015.03.001. Epub 2015 Mar 29. Adv Cancer Res. 2015. PMID: 26093899 Review.
Cited by
-
The impact of tumor microenvironment: unraveling the role of physical cues in breast cancer progression.Cancer Metastasis Rev. 2024 Jun;43(2):823-844. doi: 10.1007/s10555-024-10166-x. Epub 2024 Jan 19. Cancer Metastasis Rev. 2024. PMID: 38238542 Free PMC article. Review.
-
Prostate Cancer Stem Cells: Biology and Treatment Implications.Int J Mol Sci. 2023 Oct 4;24(19):14890. doi: 10.3390/ijms241914890. Int J Mol Sci. 2023. PMID: 37834336 Free PMC article. Review.
-
Proteomic-based stemness score measures oncogenic dedifferentiation and enables the identification of druggable targets.Cell Genom. 2025 Jun 11;5(6):100851. doi: 10.1016/j.xgen.2025.100851. Epub 2025 Apr 17. Cell Genom. 2025. PMID: 40250426 Free PMC article.
-
Application and new findings of scRNA-seq and ST-seq in prostate cancer.Cell Regen. 2024 Oct 29;13(1):23. doi: 10.1186/s13619-024-00206-w. Cell Regen. 2024. PMID: 39470950 Free PMC article. Review.
-
Metronomic chemotherapy in cancer treatment: new wine in an old bottle.Theranostics. 2024 Jun 1;14(9):3548-3564. doi: 10.7150/thno.95619. eCollection 2024. Theranostics. 2024. PMID: 38948068 Free PMC article. Review.
References
-
- Magnan S, Zarychanski R, Pilote L, Bernier L, Shemilt M, Vigneault E, et al. . Intermittent vs continuous androgen deprivation therapy for prostate cancer: a systematic review and meta-analysis. JAMA Oncol 2015;1:1261–9. - PubMed
-
- Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P, et al. . 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 2016;375:1415–24. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
