

Cardiovascular toxicity from therapies for light chain amyloidosis
- PMID: 37476571
- PMCID: PMC10354454
- DOI: 10.3389/fcvm.2023.1212983
Cardiovascular toxicity from therapies for light chain amyloidosis
Abstract
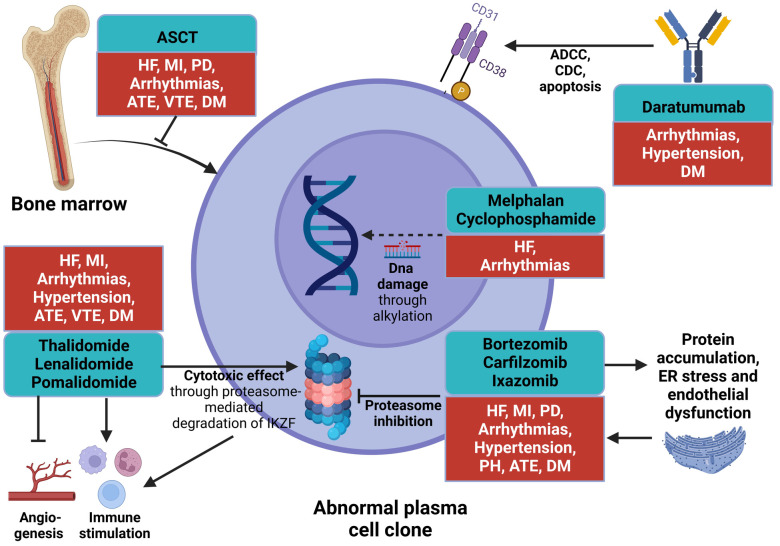
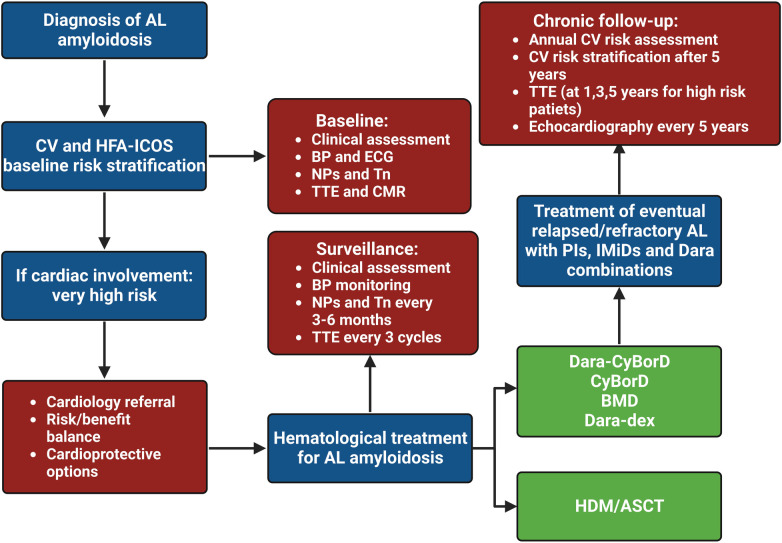
Amyloid light-chain (AL) amyloidosis is a hematological disorder characterized by abnormal proliferation of a plasma cell clone producing monoclonal free light chains that misfold and aggregate into insoluble fibrils in various tissues. Cardiac involvement is a common feature leading to restrictive cardiomyopathy and poor prognosis. Current first-line treatments aim at achieving hematological response by targeting the plasma cell clones, and these have been adapted from multiple myeloma therapy. Patients with AL amyloidosis often exhibit multiorgan involvement, making them susceptible to cancer therapy-related cardiovascular toxicity. Managing AL amyloidosis is a complex issue that requires enhanced knowledge of the cardio-oncological implications of hematological treatments. Future research should focus on implementing and validating primary and secondary prevention strategies and understanding the biochemical basis of oncological therapy-related damage to mitigate cardiovascular toxicity.
Keywords: AL amyloidosis; cardiac amyloidosis; cardiovascular toxicity; chemotherapy; treatment.
© 2023 Morfino, Aimo, Castiglione, Chianca, Vergaro, Cipolla, Fedele, Emdin, Fabiani and Cardinale.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Bringhen S, Milan A, Ferri C, Wäsch R, Gay F, Larocca A, et al. Cardiovascular adverse events in modern myeloma therapy—incidence and risks. A review from the European myeloma network (EMN) and Italian society of arterial hypertension (SIIA). Haematologica. (2018) 103(9):1422–32. 10.3324/haematol.2018.191288 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources