

A Review of Theranostics: Perspectives on Emerging Approaches and Clinical Advancements
- PMID: 37477566
- PMCID: PMC10413300
- DOI: 10.1148/rycan.220157
A Review of Theranostics: Perspectives on Emerging Approaches and Clinical Advancements
Abstract
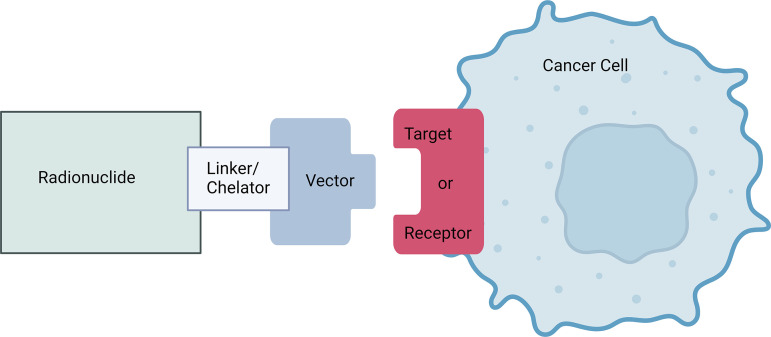
Theranostics is the combination of two approaches-diagnostics and therapeutics-applied for decades in cancer imaging using radiopharmaceuticals or paired radiopharmaceuticals to image and selectively treat various cancers. The clinical use of theranostics has increased in recent years, with U.S. Food and Drug Administration (FDA) approval of lutetium 177 (177Lu) tetraazacyclododecane tetraacetic acid octreotate (DOTATATE) and 177Lu-prostate-specific membrane antigen vector-based radionuclide therapies. The field of theranostics has imminent potential for emerging clinical applications. This article reviews critical areas of active clinical advancement in theranostics, including forthcoming clinical trials advancing FDA-approved and emerging radiopharmaceuticals, approaches to dosimetry calculations, imaging of different radionuclide therapies, expanded indications for currently used theranostic agents to treat a broader array of cancers, and emerging ideas in the field. Keywords: Molecular Imaging, Molecular Imaging-Cancer, Molecular Imaging-Clinical Translation, Molecular Imaging-Target Development, PET/CT, SPECT/CT, Radionuclide Therapy, Dosimetry, Oncology, Radiobiology © RSNA, 2023.
Keywords: Dosimetry; Molecular Imaging; Molecular Imaging–Cancer; Molecular Imaging–Clinical Translation; Molecular Imaging–Target Development; Oncology; PET/CT; Radiobiology; Radionuclide Therapy; SPECT/CT.
Conflict of interest statement
Figures
References
-
- Kendi AT , Halfdanarson TR , Packard A , Dundar A , Subramaniam RM . Therapy with 177Lu-DOTATATE: clinical implementation and impact on care of patients with neuroendocrine tumors . AJR Am J Roentgenol 2019. ; 213 ( 2 ): 309 – 317 . - PubMed
-
- Modoni S , Frangos S , Iakovou I , Boero M , Mansi L . Theragnostics before we found its name . Q J Nucl Med Mol Imaging 2021. ; 65 ( 4 ): 299 – 305 . - PubMed
-
- Chapman EM . History of the discovery and early use of radioactive iodine . JAMA 1983. ; 250 ( 15 ): 2042 – 2044 . - PubMed
-
- Kassis AI , Adelstein SJ . Radiobiologic principles in radionuclide therapy . J Nucl Med 2005. ; 46 ( Suppl 1 ): 4S – 12S . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
