

Number, Duration, and Distribution of Wake Bouts in Patients with Insomnia Disorder: Effect of Daridorexant and Zolpidem
- PMID: 37477771
- PMCID: PMC10374812
- DOI: 10.1007/s40263-023-01020-9
Number, Duration, and Distribution of Wake Bouts in Patients with Insomnia Disorder: Effect of Daridorexant and Zolpidem
Abstract
Background: Daridorexant, a dual orexin receptor antagonist approved in early 2022, reduces wake after sleep onset without reducing the number of awakenings in patients with insomnia. The objective of this post hoc analysis was to explore the effect of daridorexant on the number, duration, and distribution of night-time wake bouts, and their correlation with daytime functioning.
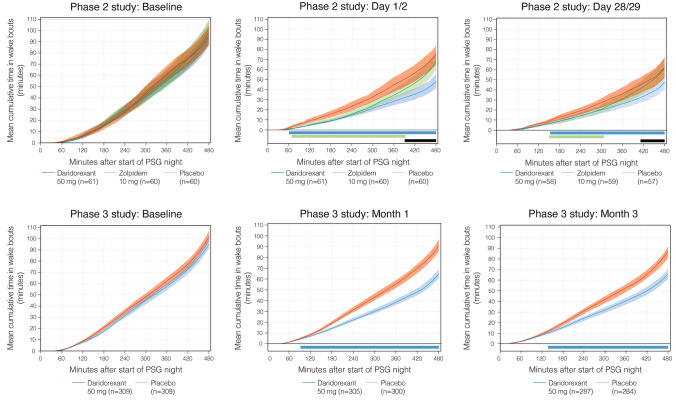
Methods: Adults with insomnia disorder were randomized 1:1:1:1:1:1 to placebo, zolpidem 10 mg, or daridorexant 5, 10, 25, or 50 mg in a phase II dose-finding study, and 1:1:1 to placebo or daridorexant 25 or 50 mg in a pivotal phase III study. We analyzed polysomnography data for daridorexant 25 and 50 mg, zolpidem 10 mg, and placebo groups. Polysomnography was conducted at baseline, then on Days 1/2, 15/16, and 28/29 in the phase II study, and Months 1 and 3 in the phase III study. The number, duration, and distribution of wake bouts (≥ 0.5 min) were assessed.
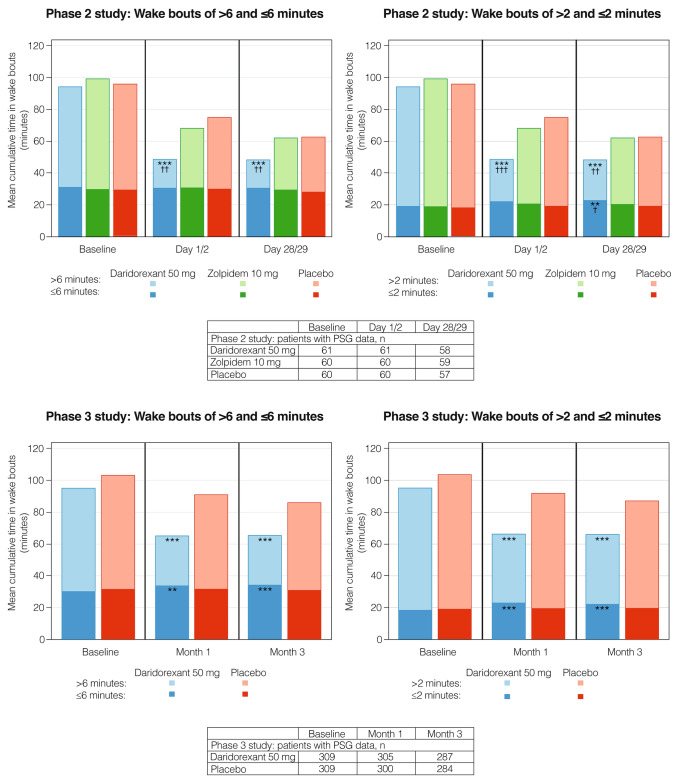
Results: Data from 1111 patients (phase II study: daridorexant 50 mg [n = 61], zolpidem 10 mg [n = 60], placebo [n = 60]; phase III study: daridorexant 25 mg [n = 310], daridorexant 50 mg [n = 310], placebo [n = 310]) were analyzed. Long wake bouts were defined as > 6 min. Compared with placebo, daridorexant 50 mg reduced overall wake time (p < 0.05; all time points, both studies), the odds of experiencing long wake bouts (p < 0.001; Months 1 and 3, phase III study), and the cumulative duration of long wake bouts (p < 0.01; all time points, both studies). Reductions in long wake bouts were sustained through the second half of the night and correlated with improvements in daytime functioning. An increase in the cumulative duration of short wake bouts was observed with daridorexant 50 mg (p < 0.01 vs placebo, Months 1 and 3, phase III study); this was uncorrelated with daytime functioning.
Conclusion: Daridorexant reduced the number and duration of longer wake bouts throughout the night compared with placebo, corresponding with improved daytime functioning.
Clinical trials: Clinicaltrials.gov NCT02839200 (registered July 20, 2016), NCT03545191 (registered June 4, 2018).
© 2023. The Author(s).
Conflict of interest statement
Financial disclosures: YD reports board membership, consultancy, and lecture activity with Idorsia Pharmaceuticals Ltd. TES and AND report consultancy and lecture activity with Idorsia Pharmaceuticals Ltd, Neurocrine, Epilog, Angelini Pharma and Jazz Pharmaceuticals. GZ is an employee of Clinilabs Drug Development Corporation, a company that has received grants from Idorsia Pharmaceuticals Ltd and reports consultancy activity with Idorsia Pharmaceuticals Ltd. TDM and MM are employees of Idorsia Pharmaceuticals Ltd. DSK was an employee of Idorsia Pharmaceuticals Ltd at the time the research was conducted. Non-financial disclosures: none.
Figures

References
-
- Hohagen F, Käppler C, Schramm E, Riemann D, Weyerer S, Berger M. Sleep onset insomnia, sleep maintaining insomnia and insomnia with early morning awakening—temporal stability of subtypes in a longitudinal study on general practice attenders. Sleep. 1994;17:551–554. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
