

Age and Sex Differences in the Genetics of Cardiomyopathy
- PMID: 37477868
- PMCID: PMC10721711
- DOI: 10.1007/s12265-023-10411-8
Age and Sex Differences in the Genetics of Cardiomyopathy
Abstract
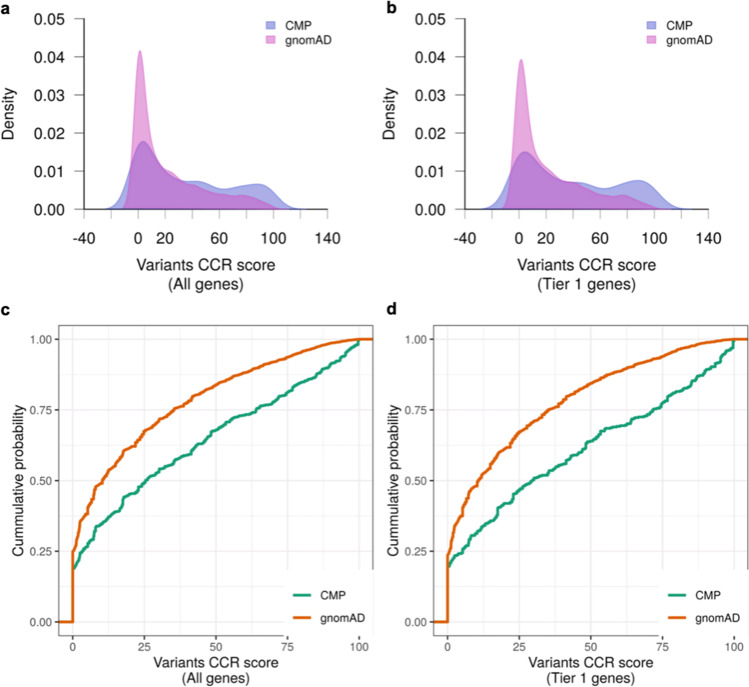
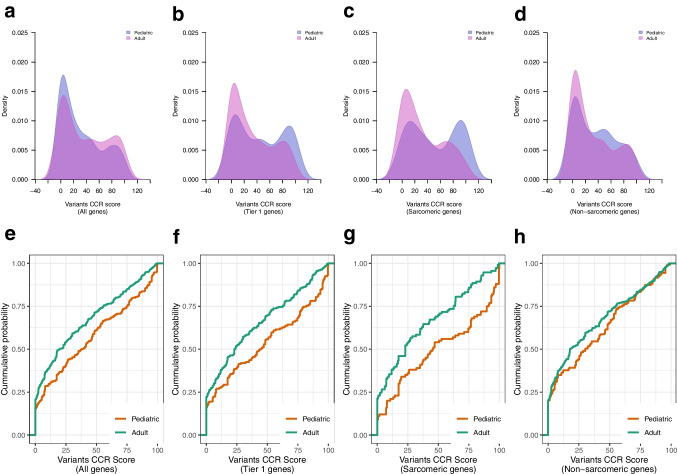
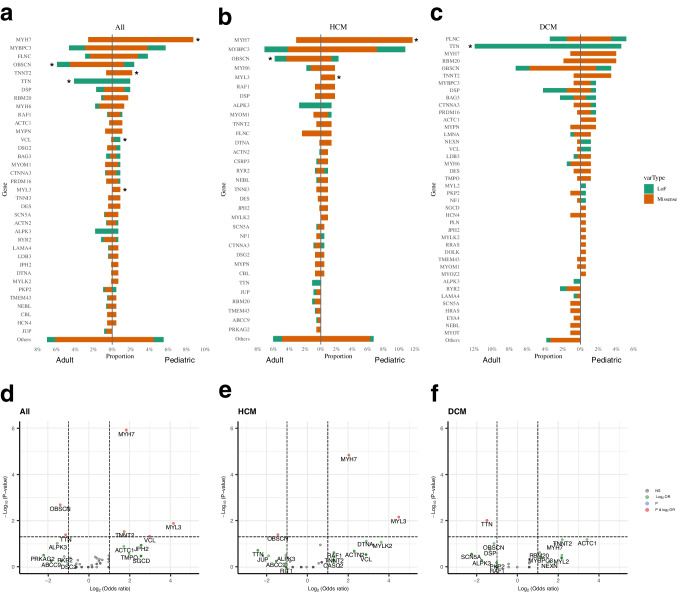
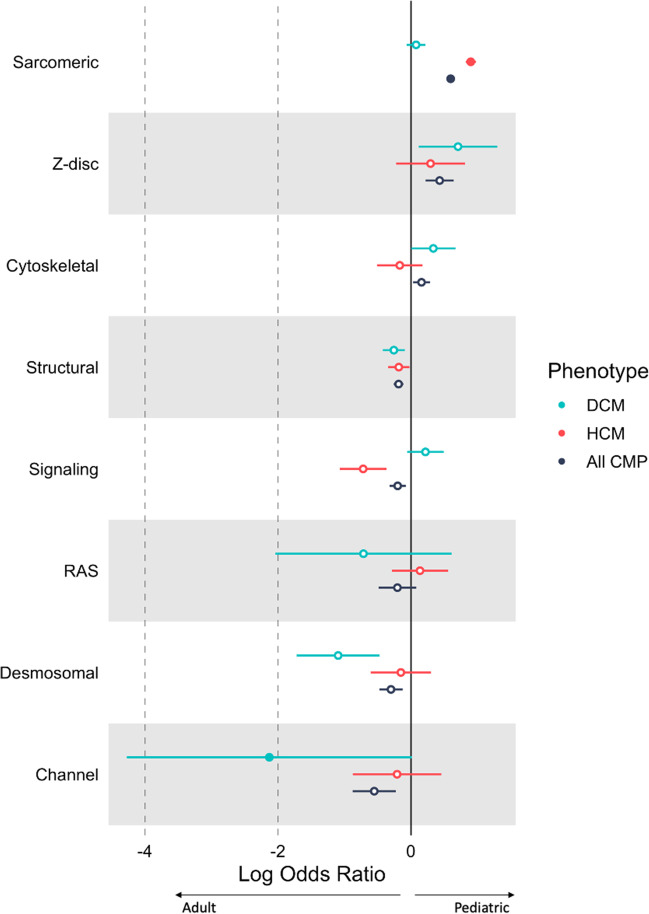
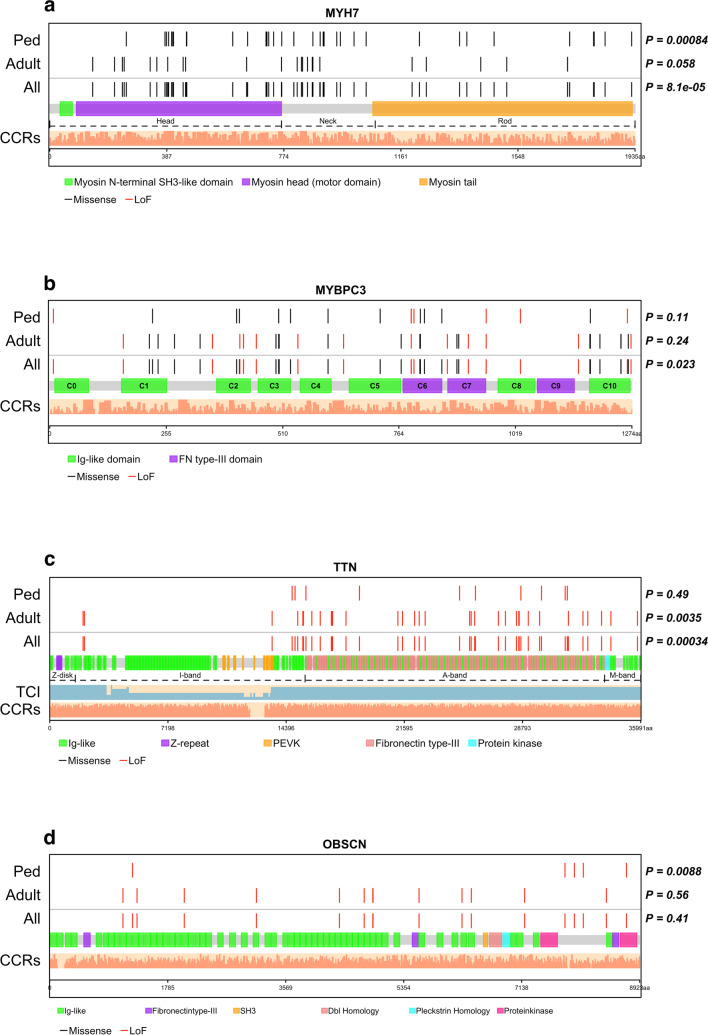
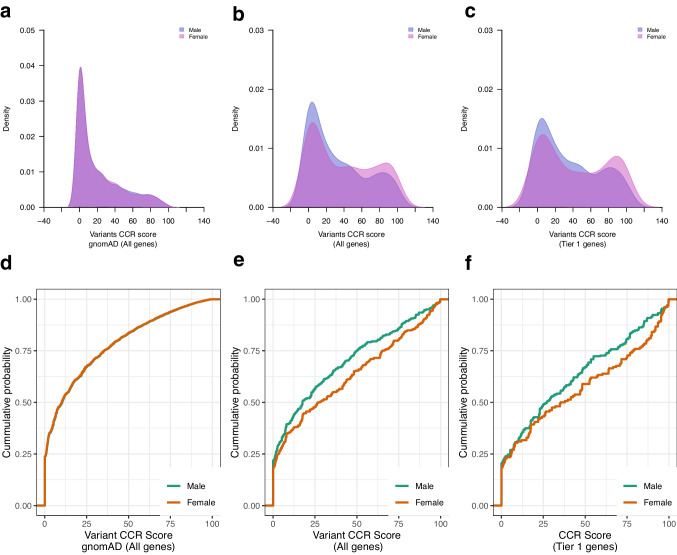
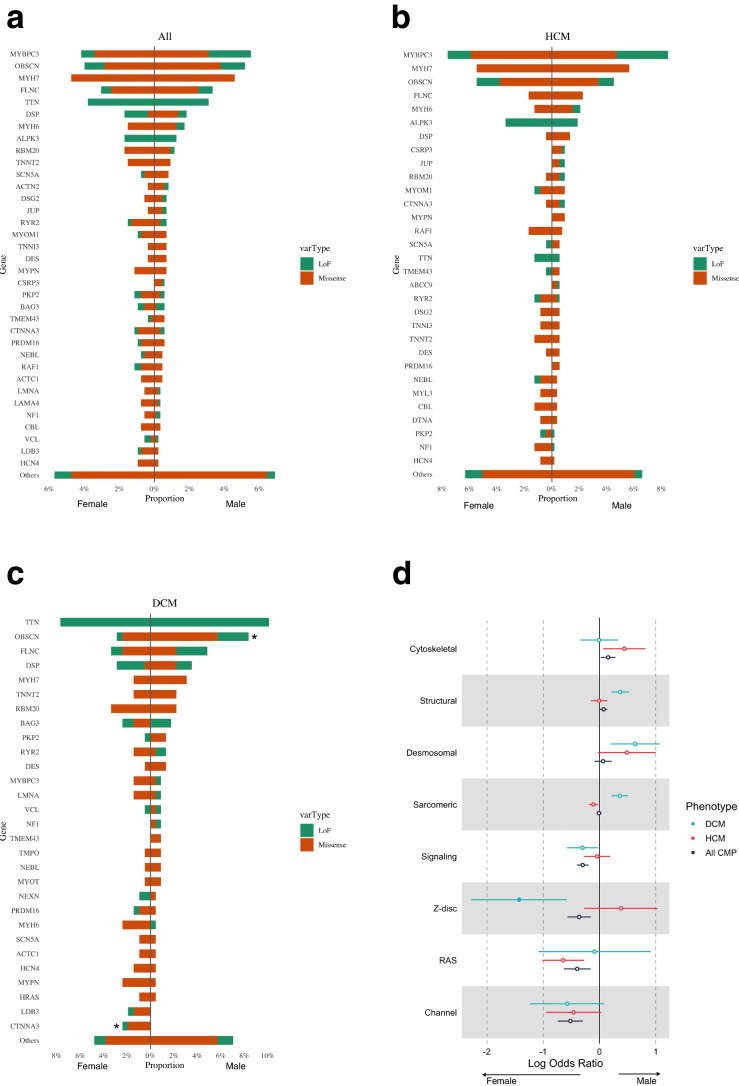
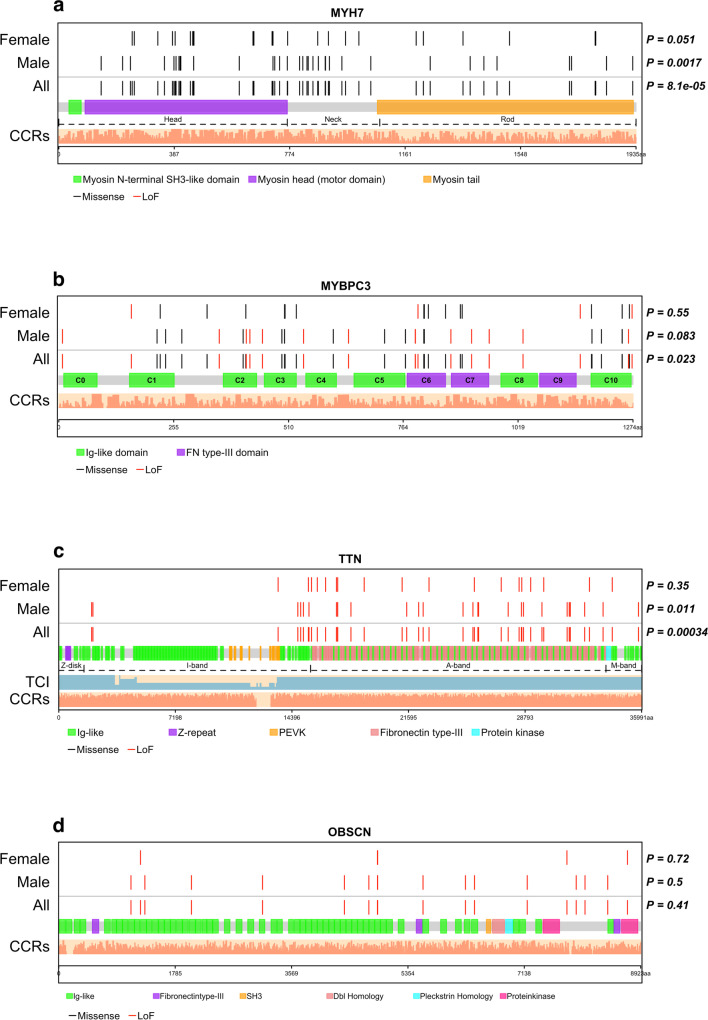
Cardiomyopathy has variable penetrance. We analyzed age and sex-related genetic differences in 1,397 cardiomyopathy patients (Ontario, UK) with whole genome sequencing. Pediatric cases (n = 471) harbored more deleterious protein-coding variants in Tier 1 cardiomyopathy genes compared to adults (n = 926) (34.6% vs 25.9% respectively, p = 0.0015), with variant enrichment in constrained coding regions. Pediatric patients had a higher burden of sarcomere and lower burden of channelopathy gene variants compared to adults. Specifically, pediatric patients had more MYH7 and MYL3 variants in hypertrophic cardiomyopathy, and fewer TTN truncating variants in dilated cardiomyopathy. MYH7 variants clustered in the myosin head and neck domains in children. OBSCN was a top mutated gene in adults, enriched for protein-truncating variants. In dilated cardiomyopathy, female patients had a higher burden of z-disc gene variants compared to males. Genetic differences may explain age and sex-related variability in cardiomyopathy penetrance. Genotype-guided predictions of age of onset can inform pre-test genetic counseling. Pediatric cardiomyopathy patients were more likely to be genotype-positive than adults with a higher burden of variants in MYH7, MYL3, TNNT2, VCL. Adults had a higher burden of OBSCN and TTN variants. Females with dilated cardiomyopathy (DCM) had a higher burden of z-disc gene variants compared to males.
Keywords: Age; Cardiomyopathy; Genetic; Genomic constraints; Sex; Whole genome sequencing.
© 2023. The Author(s).
Conflict of interest statement
SM is on the Advisory Board of Bristol Myers Squibb, and Tenaya Therapeutics. The remaining authors have nothing to disclose.
Figures
References
-
- Lipshultz SE, Law YM, Asante-Korang A, Austin ED, Dipchand AI, Everitt MD, Hsu DT, Lin KY, Price JF, Wilkinson JD, et al. Cardiomyopathy in Children: Classification and Diagnosis: A Scientific Statement From the American Heart Association. Circulation. 2019;140:e9–e68. doi: 10.1161/cir.0000000000000682. - DOI - PubMed
-
- Musunuru K, Hershberger RE, Day SM, Klinedinst NJ, Landstrom AP, Parikh VN, Prakash S, Semsarian C, Sturm AC. Genetic Testing for Inherited Cardiovascular Diseases: A Scientific Statement From the American Heart Association. Circ Genom Precis Med. 2020;13:e000067. doi: 10.1161/hcg.0000000000000067. - DOI - PubMed
-
- Ware SM, Wilkinson JD, Tariq M, Schubert JA, Sridhar A, Colan SD, Shi L, Canter CE, Hsu DT, Webber SA, et al. Genetic Causes of Cardiomyopathy in Children: First Results From the Pediatric Cardiomyopathy Genes Study. J Am Heart Assoc. 2021;10:e017731. doi: 10.1161/jaha.120.017731. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
