

Safety and Immunogenicity of a ChAd155-Vectored Respiratory Syncytial Virus Vaccine in Infants 6-7 Months of age: A Phase 1/2 Randomized Trial
- PMID: 37477875
- PMCID: PMC10786261
- DOI: 10.1093/infdis/jiad271
Safety and Immunogenicity of a ChAd155-Vectored Respiratory Syncytial Virus Vaccine in Infants 6-7 Months of age: A Phase 1/2 Randomized Trial
Abstract
Background: Respiratory syncytial virus (RSV) is a common cause of lower respiratory tract infections in infants. This phase 1/2, observer-blind, randomized, controlled study assessed the safety and immunogenicity of an investigational chimpanzee-derived adenoviral vector RSV vaccine (ChAd155-RSV, expressing RSV F, N, and M2-1) in infants.
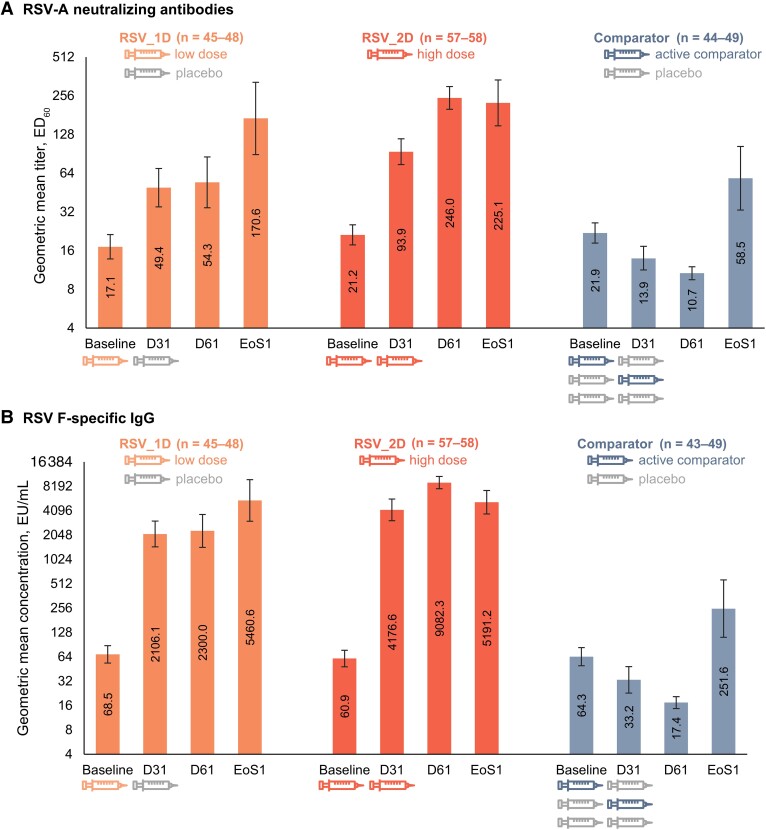
Methods: Healthy 6- to 7-month-olds were 1:1:1-randomized to receive 1 low ChAd155-RSV dose (1.5 × 1010 viral particles) followed by placebo (RSV_1D); 2 high ChAd155-RSV doses (5 × 1010 viral particles) (RSV_2D); or active comparator vaccines/placebo (comparator) on days 1 and 31. Follow-up lasted approximately 2 years.
Results: Two hundred one infants were vaccinated (RSV_1D: 65; RSV_2D: 71; comparator: 65); 159 were RSV-seronaive at baseline. Most solicited and unsolicited adverse events after ChAd155-RSV occurred at similar or lower rates than after active comparators. In infants who developed RSV infection, there was no evidence of vaccine-associated enhanced respiratory disease (VAERD). RSV-A neutralizing titers and RSV F-binding antibody concentrations were higher post-ChAd155-RSV than postcomparator at days 31, 61, and end of RSV season 1 (mean follow-up, 7 months). High-dose ChAd155-RSV induced stronger responses than low-dose, with further increases post-dose 2.
Conclusions: ChAd155-RSV administered to 6- to 7-month-olds had a reactogenicity/safety profile like other childhood vaccines, showed no evidence of VAERD, and induced a humoral immune response. Clinical Trials Registration. NCT03636906.
Keywords: ChAd155; RSV; immunogenicity; infant; vaccine-associated enhanced respiratory disease.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. V. N., Y. Z., W. P., D. F., I. D., A. G. L., R. M., S. K. S., and N. V. are or were employees of GSK during the conduct of the study. I. D., W. P., and S. K. S. hold GSK shares/stocks. R. M. and S. K. S. hold stock/stock options in Moderna. B. T., E. J. A., B. S. C., E. C. D., H. S., J. D. C., J. M. M. A., K. L., M. M. M.-P., M. R., S. N. F., F. B.-A., and T. P. report grants and/or other support from GSK for the conduct of the study. J. M. L. reports grants from GSK paid to her institution for the conduct of the study and holds the CIHR-GSK Chair in Pediatric Vaccinology at Dalhousie University. B. T. reports grants from GSK, Merck, and Pfizer for other trials. C. e. reports support for scientific meetings from GSK and ViiV and advisory consultancy fees from GSK. E. J. A. has consulted for Pfizer, Sanofi Pasteur, GSK, Janssen, Moderna, and Medscape, and his institution receives funds to conduct clinical research unrelated to this manuscript from MedImmune, Regeneron, PaxVax, Pfizer, GSK, Merck, Novavax, Sanofi Pasteur, Janssen, and Micron; he serves on a safety monitoring board for Kentucky BioProcessing and Sanofi Pasteur; serves on a data adjudication board for WCG and ACI Clinical; and his institution has also received funding from the National Institutes of Health to conduct clinical trials of COVID-19 vaccines. B. S. C. reports grants for other vaccine trials from GSK and MSD paid to his institution. E. C. D. performs contract work for the Eskisehir Osmangazi University funded by GSK, Sanofi Pasteur, and Pfizer. E. K. reports honoraria for lectures from GSK, MSD, AstraZeneca, Sanofi, and Pfizer. E. L.-M. reports grants from Centro de Estudios en Infectología Pediátrica. F. M.-T. reports grants from Janssen, MSD, and AstraZeneca; personal fees from Ablynx, GSK, Pfizer, MSD, Sanofi Pasteur, Novavax, Seqirus, and Biofabri; nonfinancial support from GSK, Pfizer, MSD, and Seqirus; and trial fees paid to his institution from these different companies (except Biofabri). H. S. reports personal fees and trial fees paid to his institution from MSD, Seqirus, Pfizer, Janssen, and Sanofi Pasteur. I. S. C. has received payment to his institution from GSK for the conduct of the study, by contract approved by the corresponding ethical committees and health authorities, and for trials of other vaccine manufacturers, and has received grants and/or honoraria as a consultant/advisor/speaker or for attending conferences and practical courses from GSK and other vaccine manufacturers. J. D. C. is a member of the Committee on Infectious Diseases of the American Academy of Pediatrics and reports funds paid to his university to study RSV vaccines. J. D.-D. reports grants from GSK, MSD, and Sanofi Pasteur paid to his institution. J. M. M. A. reports fees for medical meetings from GSK and Pfizer. K. L. reports grants from ReViral and Shionogi. M. M.-P. reports grants from MSD, Roche, GSK, Janssen, Takeda, and Syneos. M. R. reports grants for other vaccine trials from GSK and other vaccine manufacturers paid to his institution. S. N. F. reports fees paid to his institution for attending meetings, advisory boards, and/or grants for clinical trials from AstraZeneca/Medimmune, GSK, J&J, Pfizer, Sanofi, Seqirus, Sandoz, Valneva, Novavax, and Merck. X. S.-L. reports grants from Cevaxin Vaccine Research Center. F. B.-A. reports consultancy fees from GSK, Pfizer, and MSD and grants from MSD. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures



References
-
- Obando-Pacheco P, Justicia-Grande AJ, Rivero-Calle I, et al. Respiratory syncytial virus seasonality: a global overview. J Infect Dis 2018; 217:1356–64. - PubMed
