

Assessment of Meal Anticipation for Improving Fully Automated Insulin Delivery in Adults With Type 1 Diabetes
- PMID: 37478323
- PMCID: PMC10465820
- DOI: 10.2337/dc23-0119
Assessment of Meal Anticipation for Improving Fully Automated Insulin Delivery in Adults With Type 1 Diabetes
Abstract
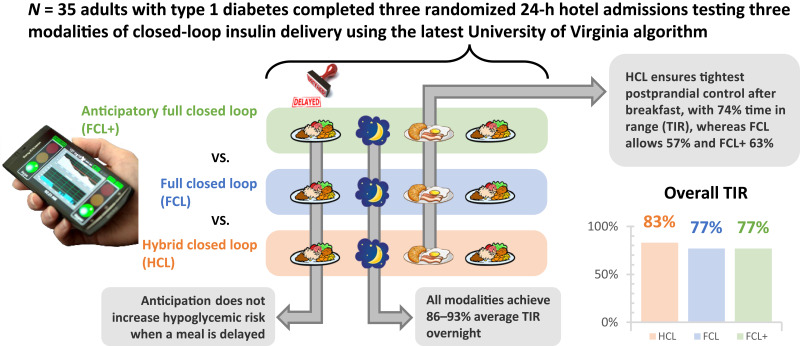
Objective: Meals are a consistent challenge to glycemic control in type 1 diabetes (T1D). Our objective was to assess the glycemic impact of meal anticipation within a fully automated insulin delivery (AID) system among adults with T1D.
Research design and methods: We report the results of a randomized crossover clinical trial comparing three modalities of AID systems: hybrid closed loop (HCL), full closed loop (FCL), and full closed loop with meal anticipation (FCL+). Modalities were tested during three supervised 24-h admissions, where breakfast, lunch, and dinner were consumed per participant's home schedule, at a fixed time, and with a 1.5-h delay, respectively. Primary outcome was the percent time in range 70-180 mg/dL (TIR) during the breakfast postprandial period for FCL+ versus FCL.
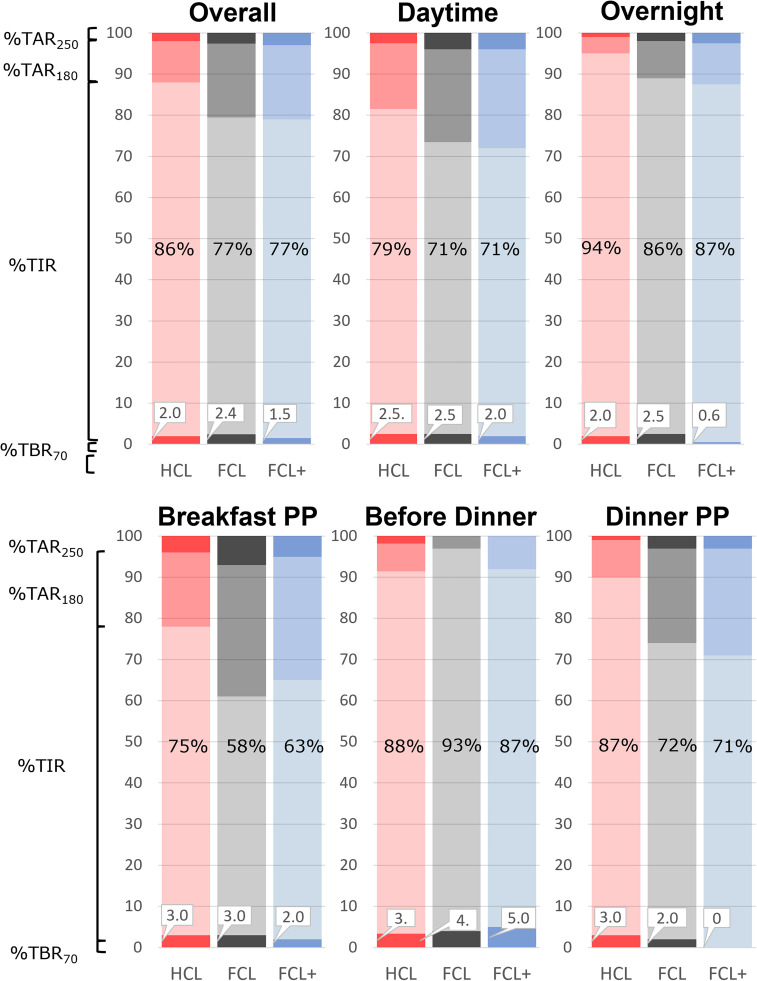
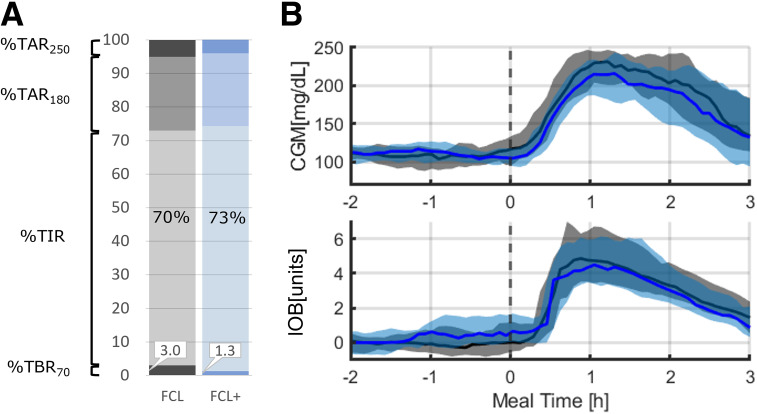
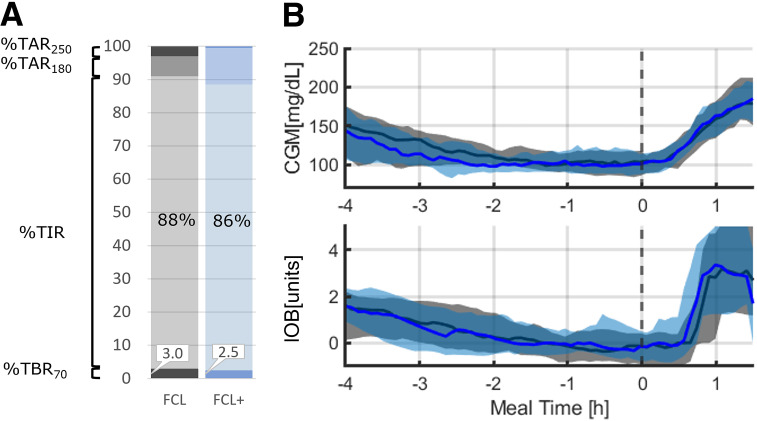
Results: Thirty-five adults with T1D (age 44.5 ± 15.4 years; HbA1c 6.7 ± 0.9%; n = 23 women and n = 12 men) were randomly assigned. TIR for the 5-h period after breakfast was 75 ± 23%, 58 ± 21%, and 63 ± 19% for HCL, FCL, and FCL+, respectively, with no significant difference between FCL+ and FCL. For the 2 h before dinner, time below range (TBR) was similar for FCL and FCL+. For the 5-h period after dinner, TIR was similar for FCL+ and FCL (71 ± 34% vs. 72 ± 29%; P = 1.0), whereas TBR was reduced in FCL+ (median 0% [0-0%] vs. 0% [0-0.8%]; P = 0.03). Overall, 24-h control for HCL, FCL, and FCL+ was 86 ± 10%, 77 ± 11%, and 77 ± 12%, respectively.
Conclusions: Although postprandial control remained optimal with hybrid AID, both fully AID solutions offered overall TIR >70% with similar or lower exposure to hypoglycemia. Anticipation did not significantly improve postprandial control in AID systems but also did not increase hypoglycemic risk when meals were delayed.
© 2023 by the American Diabetes Association.
Conflict of interest statement
Figures
References
-
- Bergenstal RM, Garg S, Weinzimer SA, et al. . Safety of a hybrid closed-loop insulin delivery system in patients with type 1 diabetes. JAMA 2016;316:1407–1408 - PubMed
